doi: 10.56294/mw2023108
ORIGINAL
Examining the Learning Outcomes of Multimedia-Assisted Instruction in Surgical Training for Medical Students
Examen de los resultados de aprendizaje de la enseñanza asistida por multimedia en la formación quirúrgica de estudiantes de medicina
Rajesh Kumar Lenka1 ![]() *, Manashree
Mane2
*, Manashree
Mane2 ![]() , Keshav3
, Keshav3 ![]()
1IMS and SUM Hospital, Siksha ‘O’ Anusandhan (deemed to be University), Department of Microbiology. Bhubaneswar, Odisha, India.
2JAIN (Deemed-to-be University), Department of Forensic science. Bangalore, Karnataka, India.
3Noida International University, Department of General Medicine. Greater Noida, Uttar Pradesh, India.
Cite as: Lenka RK, Mane M, Keshav. Examining the Learning Outcomes of Multimedia-Assisted Instruction in Surgical Training for Medical Students. Seminars in Medical Writing and Education. 2023; 2:108. https://doi.org/10.56294/mw2023108
Submitted: 05-09-2022 Revised: 17-12-2022 Accepted: 23-02-2023 Published: 24-02-2023
Editor: PhD.
Prof. Estela Morales Peralta ![]()
Corresponding Author: Rajesh Kumar Lenka *
ABSTRACT
Surgical training has traditionally relied on hands-on experience with cadavers or animal models; however, these methods have limitations, leading to the exploration of synthetic and virtual reality models as alternatives. Multimedia-assisted instruction has emerged as a promising approach for teaching complex surgical procedures, such as the design and construction of synthetic skin flaps.A total of 126 volunteer of final-year medical students were distributed at random to two groups: a control group (Ctrl grp) (n=63), which studied a text-based article, and a test group (Test grp) (n=63), which used multimedia software to learn how to create a rhomboid synthetic skin flap. Both groups then performed a synthetic skin flap procedure on a training bench model. IBM SPSS Statistics 25.0 was used to do the statistical analysis, with paired t-tests to contrast pre-and post-test results, and independent t-tests to compare the performance among the two groups. Test grp demonstrated significantly better performance, with higher objective checklist scores, global assessments, procedural accuracy, time taken to complete the procedure, and confidence levels in performing the procedure (p < 0,05), contrasted to the Ctrl grp. Multimedia-assisted instruction significantly enhances both subjective and objective learning outcomes in surgical training for medical students, particularly when using synthetic skin flap models. These findings support the adoption of multimedia tools for teaching complex surgical procedures.
Keywords: Multimedia; Surgical Training; Synthetic Skin Flap; Medical Students; Complex Surgical Procedures.
RESUMEN
La formación quirúrgica se ha basado tradicionalmente en la experiencia práctica con cadáveres o modelos animales; sin embargo, estos métodos tienen limitaciones, lo que ha llevado a explorar los modelos sintéticos y de realidad virtual como alternativas. Un total de 126 estudiantes voluntarios de último curso de medicina fueron distribuidos aleatoriamente en dos grupos: un grupo de control (Ctrl grp) (n=63), que estudió un artículo basado en texto, y un grupo de prueba (Test grp) (n=63), que utilizó software multimedia para aprender a crear un colgajo de piel sintética romboidal. A continuación, ambos grupos realizaron un procedimiento de colgajo de piel sintética en un modelo de banco de entrenamiento. Se utilizó IBM SPSS Statistics 25.0 para realizar el análisis estadístico, con pruebas t pareadas para contrastar los resultados previos y posteriores a la prueba, y pruebas t independientes para comparar el rendimiento entre los dos grupos. El grupo de prueba demostró un rendimiento significativamente mejor, con puntuaciones más altas en la lista de comprobación objetiva, evaluaciones globales, precisión del procedimiento, tiempo necesario para completar el procedimiento y niveles de confianza en la realización del procedimiento (p < 0,05), en contraste con el grupo Ctrl. La instrucción asistida por multimedia mejora significativamente los resultados de aprendizaje subjetivos y objetivos en la formación quirúrgica de los estudiantes de medicina, en particular cuando se utilizan modelos de colgajo de piel sintética. Estos resultados respaldan la adopción de herramientas multimedia para la enseñanza de procedimientos quirúrgicos complejos.
Palabras clave: Multimedia; Formación Quirúrgica; Colgajo de Piel Sintética; Estudiantes de Medicina; Procedimientos Quirúrgicos Complejos.
INTRODUCTION
An important component of medical education is surgical training, which traditionally depended on mentorship, hands-on experience, and direct observation. However, medical students might struggle to acquire important surgical skills because of the limitations of traditional methods, including patient access, stressful work environments, and time constraints.(1) The complexity of advanced surgeries further complicates the training process, leaving medical students to learn an immense number of techniques and concepts within a comparatively limited period.(2) New developments in medical education, like virtual patients,e-learning, and simulations, have emerged to facilitate an active, student-centered pedagogy.(3) Technological advancements have greatly influenced human-computer interaction (HCI) and education, enhancing evaluation, engagement, and learning. Virtual reality (VR) has transformed HCI by offering novel insights and involving users. The trend has also dominated the medical education field, and VR-based simulations have been employed in medical specialties such as arthroscopic, cardiac, and laparoscopic surgery.(4) This has enabled more immersive and realistic learning environments, where students can deal with 3D models and rehearse surgical procedures numerous times, making their skills better in a controlled environment.(5) Surgeons and residents are increasingly applying VR simulators in medical university training to analyze, propose, and compare possible surgical interventions to different medical diseases. This aids in overcoming the limitations of current training methods.(6) Many training facilities, including internet access and mobile electronic devices, are currently accessible to medical professionals. These resources can reshape conventional, personalized learning into a shared, international, and collective education, lessening the control of educational potentiality and formation sites over residents and experts.(7) More realistic simulation has been facilitated through the integration of VR and augmented reality (AR) technology into surgical teaching, enhancing the student's competence in procedures such as tissue dissection, suturing, and instrument manipulation.(8)
A hybrid surgical simulator that combined virtual and real-world elements for laparoscopic cholecystectomy was introduced.(9) The simulator tracks the laparoscope and target anatomy using an electromagnetic field generator, and it also has a second camera for video tracking. The hardware robustness, realism, and correctness of the simulator were assessed. The simulator satisfies the initial requirements in terms of cost reduction, modularity, reusability, and anatomical appearance. Learning how to recognize and isolate Calot's triangle during laparoscopic cholecystectomy and other surgical procedures could be a useful training aid. VR and AR have been used in surgical training to help inexperienced residents who are hesitant to conduct big surgeries.(10) The way surgical residents' knowledge and self-confidence were affected by virtual reality surgery was assessed. A control group (Ctrl grp) and a study group of 95 residents from seven dental schools participated. The studies group's perceived self-confidence levels were noticeably greater than those of the Ctrl grp, and the most gain was shown during the first training year. The application of Computer-Based Video Instruction (CBVI) in dermatology procedure instruction for medical students was examined in this pilot project. (11) 33,3 % of students said that the experience heightened participants' interest in the topic, and the CBVI group outperformed the other group in shave and punch biopsies. Adding CBVI to the dermatological curriculum improved students' procedural knowledge and sparked their interest in the subject.Opposed to traditional group viewing, self-paced video tutorial viewingenhanced theacquisition of surgical skills among interns in obstetrics and gynecology.(12) Video tutorials were used to teach 35 Obstetrics and Gynecology (OBGYN PGY-1) trainees the fundamentals of open surgery. The findings revealed no discernible difference among group and self-paced viewing in terms of workload stress or competency scores. According to the research, self-paced watching might be a more successful way to help interns develop their surgical abilities.
22 general surgery residents participated by executing an intestinal anastomosis on camera.(13) While the ctrl grp carried on with their usual tasks, the self-directed learning group via video was given expert videos. There was no discernible dissimilarity in the residents' scores across the groups following a second filmed anastomosis. Before and following the intervention, both groups showed considerable improvement; however, the intervention group's final Objective Structure Assessment of Technical Skills (OSATS) score was greater. Using videos for self-directed learning did not considerably raise OSATS scores overall.The efficacy of online surgical skills electives for medical students of undergraduate was evaluated.(14) The one-week online training covered suturing, knot tying, and surgical instrument identification. 86 students participated and the results demonstrated that the elective enhanced students' knowledge, abilities, and confidence while offering personalized video conference feedback from peers and professionals.The outcome of surgical simulation and video instruction on the procedural abilities of dermatology residents was evaluated.(15) Thirty-one dermatology residents in their first and second years from three institutions participated. Traditional lectures were replaced by at-home educational video viewing under the flipped classroom model. Residents' overall OSATS score and self-reported confidence in surgical competence both improved following three practical sessions with virtual skin models. According to the findings, procedural skills can be effectively improved through simulation and video instruction.
Evaluation of the efficacy of multimedia-assisted surgical training for medical students is the main aim. If interactive digital tools improve procedural accuracy, confidence, and overall performance in performing synthetic skin flap methods, the analysis will compare learning outcomes between a Test group (Text grp) and a Ctrl grp.
Organization of the analysis: The next part explains the methodology section and then the result was provided. The final section gives the discussion and conclusion of the analysis.
METHOD
The design of the research, participant allocation, teaching strategies, questionnaire creation, outcome measures, and statistical analysis are all covered in this section. The differences between text-based and multimedia-assisted learning in surgical training were described, as well as the statistical tests that are used to assess learning outcomes and assessment criteria, including procedural correctness and confidence levels. Figure 1 gives the overall methodology flow.
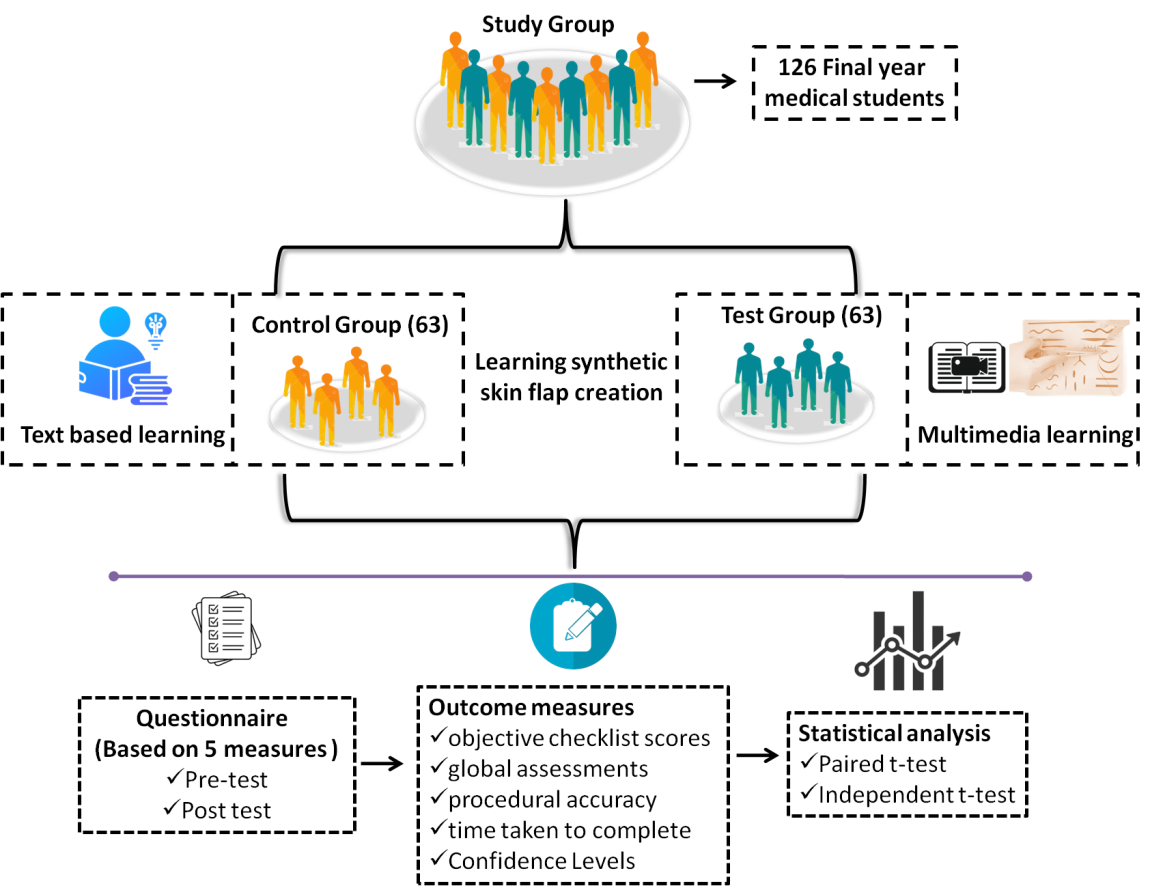
Figure 1. Flow of methodology
Research design
A Randomized Controlled Experiment (RCT) was planned to find out how effective standard text-based learning is compared to multimedia-supported training in the lubrication of rhomboid synthetic skin flaps. Participants were randomized either into the Test grp, which used interactive computer software for studying, or the Ctrl grp, which studied a text-based article. Both groups of participants were trained before performing the treatment on a model of a synthetic skin flap.
Participants
A total of 126 final-year medical students participated. The participants were equally and randomly allocated to two groups: a Ctrl grp (n = 63) that undergoes text-based instruction and a Test grp (n = 63) that employs interactive multimedia-assisted instruction. Participants' baseline characteristics were similar for age, gender distribution, and previous surgical exposure. Random allocation ensured the equivalence of groups to minimize potential bias. The 126 participants details are belikely explained in table 1.
|
Table 1. Participants’ demographic details |
|||
|
|
Characteristic |
Ctrl Grp (n=63) |
Test Grp (n=63) |
|
Age Categories |
21-23 years |
35 (55,6 %) |
36 (57,1 %) |
|
|
24-26 year |
18 (28,6 %) |
17 (26,9 %) |
|
|
27+ years |
10 (15,9 %) |
10 (15,9 %) |
|
Gender |
Female |
31 (49,2 %) |
32 (50,8 %) |
|
|
Male |
32 (50,8 %) |
31 (49,2 %) |
|
Educational Background |
Undergraduate Medical Program |
63 (100 %) |
63 (100 %) |
|
Additional Surgical Workshops or Courses |
Yes |
20 (31,7 %) |
22 (34,9 %) |
|
|
No |
43 (68,3 %) |
41 (65,1 %) |
|
Prior Surgical Experience |
No Experience |
41 (65,1 %) |
40 (63,5 %) |
|
|
Minimal Experience |
16 (25,4 %) |
17 (27,0 %) |
|
|
Moderate Experience |
6 (9,5 %) |
6 (9,5 %) |
|
Prior Exposure to Multimedia Tools |
Experienced |
30 (47,6 %) |
32 (50,8 %) |
|
|
No Experience |
33 (52,4 %) |
31 (49,2 %) |
Ctrl grp
The Ctrl grp included 63 final-year medical students who were trained with a conventional, text-based learning approach. Students learned a written article that contained step-by-step procedures for constructing a rhomboid synthetic skin flap. This group was not provided with any multimedia or interactive elements throughout their training. The Ctrl grp was formed to act as a baseline for comparing the efficacy of multimedia-supported instruction, gaining an understanding of how text-based learning affects the learning of surgical skills and knowledge.
Test grp
The Test grp, which included 63 medical students in their final year, learned how to make a rhomboid synthetic skin flap with the help of multimedia-assisted instruction. Interactive software was the instructional method employed, which involved presenting the technique through visual images, animations, and teaching videos, enabling the students to go through the learning material more interactively and engagingly. This subgroup was established to measure if multimedia software increases learning procedures compared to textual techniques with the emphasis placed on skill learning, confidence, and procedural fluency.
Questionnaire design
The questionnaire that was filled out by the participants was intended to measure different elements of their learning experience and performance, according to the objective checklist scores, global assessments, procedural accuracy, time taken to complete, and confidence levels in performing the procedure. The questionnaire was structured under these main measures, with three questions for each measure. The participants utilized a 5-point Likert scale (1 = Strongly Disagree to 5 = Strongly Agree) to score their answers. The questionnaires were administered directly after the post-test, which was administered after hands-on procedure, to get the thoughts of the participants regarding their learning experience. Pre-test was also administered prior to the intervention to measure baseline knowledge and self-assessed confidence levels so that changes can be compared subsequent to training.
Performance Indicator
Each of the parameters below is designed to provide a general view of the participants' performance, from technical competence to subjective evaluation, giving a multi-dimensional view of their learning achievement.
· Object checklist score: Indicates the degree to which participants followed detailed steps required for performing the synthetic skin flap surgery. The checklist tends to include a series of significant activities and competencies, which the learner should be able to exhibit, such as cutting incisions, proper positioning of flaps, and compliance with right surgical practices. Participants were scored for adherence to these steps, and scores reflect the degree of completeness and accuracy with which they carried out the procedure.
· Global assessments: Evaluate the overall quality of the process from a broad perspective. Both the trainer's assessment and self-assessment of the participant are incorporated. It considers the overall performance, technical ability, and capability to work under conditions that are close to actual life surgery. Subjective gradings, such as how well the trainee performed on the procedure as a whole, rather than evaluating steps individually, are common in this assessment.
· Procedural Accuracy: Procedural accuracy determines the extent to which the performance of the participant conforms to the ideal procedure. Procedural accuracy considers the extent to which the steps were followed exactly, the accuracy of the techniques used, and whether the result was in line with standards. Accuracy may include evaluating the surgical accuracy, proper use of anatomical knowledge, and the prevention of errors in the procedure.
· Time Taken to Complete the Procedure: Assess the time with which the procedure was completed. The participants were questioned regarding how long participants felt it took to complete the task. Efficiency in time for surgical procedures is important since having the capability of completing tasks within an ideal amount of time matters in real life. This also indicates the learner's comfort with the process and his/her capability to work within time limits.
· Confidence Levels in Performing the Procedure: Confidence levels measure the level of confidence the participant feels about performing the procedure on their own after training. The self-reported measurement captures the learner's perceived readiness to execute the procedure in the clinical environment. Confidence levels also assists in determining how the learning mode (text-based or multimedia) affects the confidence of the trainee, which is vital for improving clinical outcomes and patient care.
Statistical analysis
IBM SPSS Statistics 25.0 was utilized to carry out the statistical analysis. The tests conducted are listed and explained below.
Paired t-test:When the same subjects are measured at different times, it is employed to compare two related groups' means. The pre-and post-test results for both (Ctrl and Test grp) in this research were analyzed. Paired t-test was utilized specifically to establish if the performance of the participants (e.g., procedural accuracy or confidence levels) significantly improved after the instructional intervention. Equation (1) gives the mathematical formation of the Paired t-test.
![]()
Where d ̅ and sd- Mean (Mn) and Standard deviation (SD) of the dissimilarity between paired observations, and n- Number of pairs.
Independent sample t-test:Conducted to establish whether the Mn of two groups, namely Ctrl grp and Test grp, differed significantly in terms of performance after the intervention. The test measured objective checklist scores, procedural accuracy, duration to complete the procedure, and confidence levels. A significant finding showed that multimedia-assisted or text-based instructional approaches yielded better results. Equation (2) gives the mathematical formation of the independent sample t-test.
Where X ̅1, X ̅2- Mn of Test and Ctrl grps, s12, s22- Variance of Test and Ctrl grps, and n1 and n2 - Number of participants in Test and Ctrl grps.
RESULTS
Independent sample t-tests were used to evaluate the dissimilarity between the Test and Ctrl Grps and paired t-tests to contrast pre and post-test scores in each group. To ascertain the effect of interactive learning techniques, these analyses look at several performance indicators, such as confidence levels, efficiency, and skill acquisition.
Paired T-test
The Paired t-test (table 2) was carried out to contrast test scores within each group to assess the learning gains from training. The Test grp showed a significantly larger improvement across all measured outcomes compared to the Ctrl grp. Objective checklist scores increased by 17 points in the Test grp (p < 0,05), compared to only a 5-point increase in the Ctrl grp (p = 0,05), indicating superior skill acquisition. The global assessment scores and procedural accuracy also improved significantly in the Test grpat p < 0,05, while the Ctrl grp showed only modest gains. Additionally, completion time decreased more significantly in the Test grp (p < 0,05), reflecting improved efficiency in performing the surgical task. The most striking difference was observed in confidence levels, where the Test grp showed a greater increase (p < 0,05), suggesting that interactive multimedia enhances both competence and self-assurance in surgical procedures.
|
Table 2. Result of Paired t-test (Pre vs. post-test in each group |
||||||||
|
Outcome Measure |
Ctrl Grp |
Test Grp |
||||||
|
Pre-Test |
Post-Test |
p-value |
t-value |
Pre-Test |
Post-Test |
p-value |
t-value |
|
|
Mean ± SD |
Mean ± SD |
|||||||
|
Objective Checklist Score |
60 ± 5 |
65 ± 4 |
0,001 |
-3,42 |
58 ± 4 |
75 ± 3 |
<0,001 |
-8,92 |
|
Global Assessment |
3,2 ± 0,8 |
3,6 ± 0,7 |
0,039 |
-2,10 |
3,3 ± 0,7 |
4,2 ± 0,5 |
<0,001 |
-7,52 |
|
Procedural Accuracy |
55 ± 7 |
60 ± 6 |
0,008 |
-2,71 |
54 ± 6 |
72 ± 5 |
<0,001 |
-9,87 |
|
Time to Completion |
15,5 ± 2,0 |
13,2 ± 1,7 |
0,001 |
3,46 |
16,0 ± 2,1 |
10,4 ± 1,5 |
<0,001 |
9,29 |
|
Confidence Level |
2,9 ± 0,6 |
3,3 ± 0,5 |
0,006 |
-2,88 |
3,0 ± 0,5 |
4,1 ± 0,4 |
<0,001 |
-11,15 |
The performance of the Ctrl grp on five outcome measures, pre and post-test, is shown in figures 2(a) and 2(b). Although there are some post-test increases, especially in procedural accuracy and confidence levels, overall development is yet modest, indicating that the intervention had little effect on improving efficiency and ability.
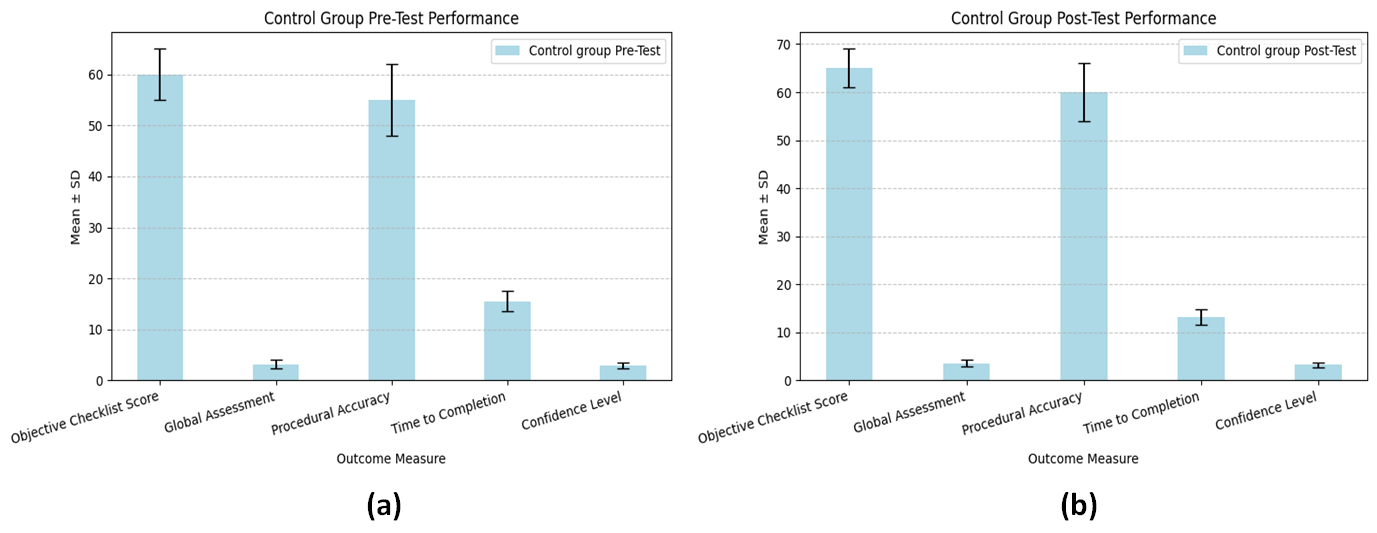
Figure 2. Ctrl grp performance (a) Pre-test (b) Post-test
The pre and post-test findings for the Test grp are shown in figures 3(a) and 3(b). All the measures, such as procedural accuracy, objective checklist scores, and confidence levels, reveal significant improvement after the test. The success of the training intervention is proved by the reduction in time to completion, which further indicates improved efficiency.
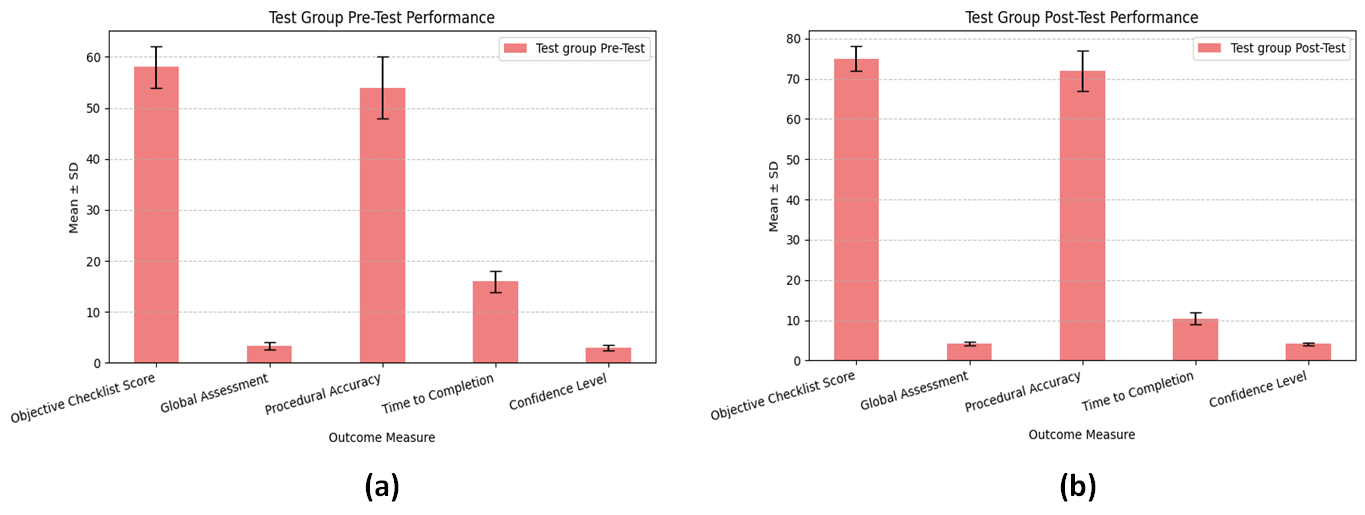
Figure 3. Test grp performance (a) Pre-test (b) Post-test
Independent sample T-test
Table 3 indicates that the Test grp outperformed the Ctrl grp on every criterion measured. In particular, the Test grp had higher objective checklist scores (p < 0,002), improved global measures (p = 0,017), and higher procedural precision (p < 0,005), supporting that the interactive software offered an improved learning process. Moreover, the Test grp participants finished the procedure much quicker (p < 0,01), showing enhanced efficiency, and also indicated a greater confidence level in executing the procedure (p < 0,03). These findings suggest that multimedia-assisted instruction enhances both technical proficiency and self-confidence compared to traditional text-based learning. Figure 4 presents the mean values and SD of outcome measures for the Ctrl and Test grp based on this test analysis to demonstrate the improved efficiency and skill proficiency of the Test grp.
|
Table 3. Result ofIndependent sample t-test (Ctrl vs. Test grp) |
||||
|
Outcome Measure |
Ctrl Grp |
Test Grp |
t-value |
p-value |
|
Mean ± SD |
||||
|
Objective Checklist Score |
65,8 ± 8,5 |
78,2 ± 7,9 |
3,12 |
< 0,002 |
|
Global Assessment |
3,8 ± 0,6 |
4,4 ± 0,5 |
2,41 |
0,017 |
|
Procedural Accuracy |
67,5 ± 7,2 |
81,3 ± 6,8 |
2,89 |
< 0,005 |
|
Time to Completion |
18,4 ± 2,5 |
15,1 ± 2,1 |
2,75 |
< 0,01 |
|
Confidence Level |
3,5 ± 0,8 |
4,2 ± 0,7 |
2,18 |
< 0,03 |
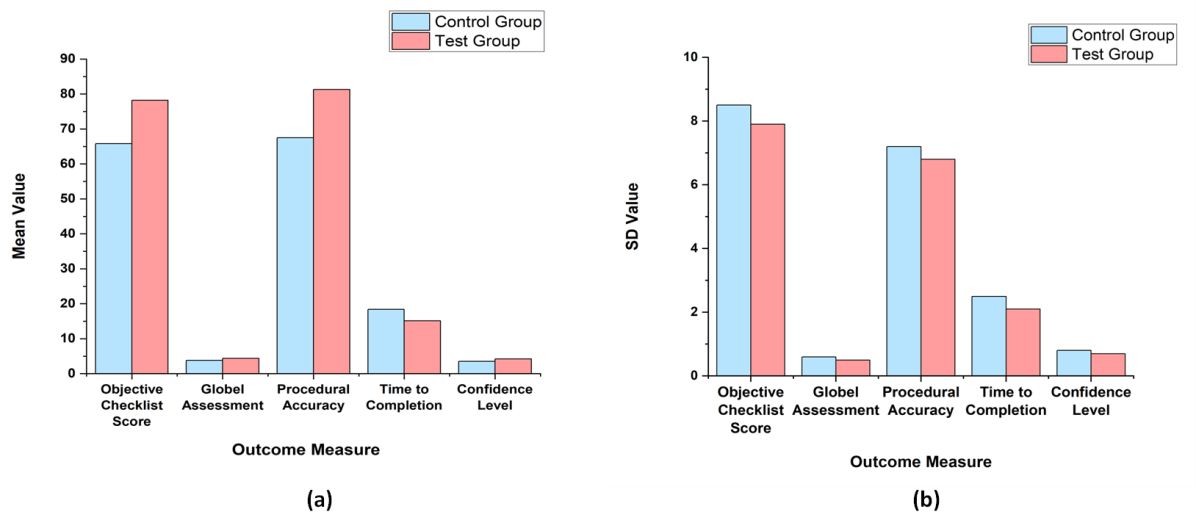
Figure 4. Group comparison based on (a) Means (b) SD
Overall, these results strongly support the use of multimedia-assisted instruction as a more effective training method for improving both objective performance and subjective confidence in surgical training compared to traditional text-based methods.
DISCUSSION
Multimedia-assisted learning effectiveness can improve surgical training outcomes for a medical student. The findings show that students who utilized interactive multimedia software outperformed those who used conventional text-based study tools by a wide margin. Multimedia-based learning is a more effective and interesting way to teach surgery, as evidenced by the enhanced global assessments, higher objective checklist scores, increased procedural accuracy, and shorter time to finish. Additionally, the notable rise in confidence among students in the Test grp implies that interactive tools make students feel more competent and prepared for conducting surgical operations, to improving technical skills. The results are consistent with earlier studies supporting the utilization of technology to improve learning in medical education, especially for skill-based training. The increased productivity seen in the group with multimedia support lends credence to the inclusion of virtual models and interactive simulations in medical education, which may lessen reliance on cadaver-based instruction. However, even if multimedia teaching has many benefits, its application should be maximized by making sure it is usable, accessible, and in line with the development of practical skills.
CONCLUSIONS
Medical students' subjective and objective learning results in surgical training are greatly improved by multimedia-assisted education, especially when synthetic skin flap models are used. Students trained with multimedia tools had better overall assessments(p = 0,017), superior checklist scores(p < 0,002), and higher procedural accuracy (p < 0,005) than the text-based learning group. The Test grp also showed higher confidence levels in completing the task (p < 0,03) and finished the operation in a significantly shorter amount of time (p < 0,01). The efficiency of multimedia-assisted education was further validated by post-test results, which demonstrated statistically significant development(p < 0,001) when contrasted to the Ctrl grp. These results are reliable that advocate using technology-enhanced learning to better surgical procedure comprehension, retention, and practical execution. The findings emphasize the necessity of including multimedia-assisted tools in medical education programs, especially for intricate surgical procedures demanding accuracy and spatial awareness. Future research should compare other multimedia forms (such as VR and AR), look at long-term memory, and evaluate how they affect actual surgical performance. Firmly supports the utilization of multimedia-based training to develop surgical skills among medical students, despite several limitations, including sample size (n = 126) and differences in prior experience.
BIBLIOGRAPHIC REFERENCES
1. Sachdeva AK. Preceptoring, proctoring, mentoring, and coaching in surgery. Journal of Surgical Oncology. 2021 Oct;124(5):711-21. 10.1002/jso.26585
2. Bjerrum F, Thomsen AS, Nayahangan LJ, Konge L. Surgical simulation: current practices and future perspectives for technical skills training. Medical teacher. 2018 Jul 3;40(7):668-75. https://doi.org/10.1080/0142159X.2018.1472754
3. Moran J, Briscoe G, Peglow S. Current technology in advancing medical education: perspectives for learning and providing care. Academic psychiatry. 2018 Dec;42:796-9. https://doi.org/10.1007/s40596-018-0946-y
4. Sattar MU, Palaniappan S, Lokman A, Hassan A, Shah N, Riaz Z. Effects of virtual reality training on medical students’ learning motivation and competency. Pakistan journal of medical sciences. 2019 May; 35(3):852. https://doi.org/10.12669/pjms.35.3.44
5. Ganry L, Hersant B, Bosc R, Leyder P, Quilichini J, Meningaud JP. Study of medical education in 3D surgical modeling by surgeons with free open-source software: Example of mandibular reconstruction with fibula free flap and creation of its surgical guides. Journal of stomatology oral and maxillofacial surgery. 2018 Sep 1;119(4):262-7. https://doi.org/10.1016/j.jormas.2018.02.012
6. Mota P, Carvalho N, Carvalho-Dias E, Costa MJ, Correia-Pinto J, Lima E. Video-based surgical learning: improving trainee education and preparation for surgery. Journal of surgical education. 2018 May 1; 75 (3):828-35. http://dx.doi.org/10.1016/j.jsurg.2017.09.027
7. Cecil J, Gupta A, Pirela-Cruz M. An advanced simulator for orthopedic surgical training. International journal of computer assisted radiology and surgery. 2018 Feb;13:305-19. https://doi.org/10.1007/s11548-017-1688-0
8. Goh GS, Lohre R, Parvizi J, Goel DP. Virtual and augmented reality for surgical training and simulation in knee arthroplasty. Archives of orthopaedic and trauma surgery. 2021 Dec;141:2303-12. https://doi.org/10.1007/s00402-021-04037-1
9. Viglialoro RM, Esposito N, Condino S, Cutolo F, Guadagni S, Gesi M, Ferrari M, Ferrari V. Augmented reality to improve surgical simulation: Lessons learned towards the design of a hybrid laparoscopic simulator for cholecystectomy. IEEE Transactions on Biomedical Engineering. 2018 Nov 28;66(7):2091-104. https://doi.org/10.1109/TBME.2018.2883816
10. Pulijala Y, Ma M, Pears M, Peebles D, Ayoub A. Effectiveness of immersive virtual reality in surgical training—a randomized control trial. Journal of Oral and Maxillofacial Surgery. 2018 May 1;76(5):1065-72. https://doi.org/10.1016/j.joms.2017.10.002
11. Cervantes J, Costello CM, Maarouf M, Kurtzman DJ, Shi VY. Computer-based video instruction for training medical students on skin biopsies. Dermatologic Surgery. 2019 Jun 1;45(6):811-7. 10.1097/DSS.0000000000001670
12. Chen LX, Fuller T, Mclntire DD, Kho KA. Introduction to open surgical skills curriculum: randomized trial of self-paced vs group video tutorial viewing. Journal of surgical education. 2019 Mar 1;76(2):453-8. https://doi.org/10.1016/j.jsurg.2018.08.019
13. Chartrand G, Soucisse M, Dubé P, Trépanier JS, Drolet P, Sideris L. Self-directed learning by video as a means to improve technical skills in surgery residents: a randomized controlled trial. BMC medical education. 2021 Dec;21:1-8. https://doi.org/10.1186/s12909-021-02524-y
14. McGann KC, Melnyk R, Saba P, Joseph J, Glocker RJ, Ghazi A. Implementation of an e-learning academic elective for hands-on basic surgical skills to supplement medical school surgical education. Journal of surgical education. 2021 Jul 1;78(4):1164-74. https://doi.org/10.1016/j.jsurg.2020.11.014
15. Liu KJ, Tkachenko E, Waldman A, Boskovski MT, Hartman RI, Levin AA, Nguyen BM, Ruiz ES, Sharon VR, Sowerby L, Tiger J. A video-based, flipped classroom, simulation curriculum for dermatologic surgery: a prospective, multi-institution study. Journal of the American Academy of Dermatology. 2019 Dec 1;81(6):1271-6. https://doi.org/10.1016/j.jaad.2019.03.078
FINANCING
None.
CONFLICT OF INTEREST
Authors declare that there is no conflict of interest.
AUTHORSHIP CONTRIBUTION
Conceptualization: Rajesh Kumar Lenka, Manashree Mane, Keshav.
Data curation: Rajesh Kumar Lenka, Manashree Mane, Keshav.
Formal analysis: Rajesh Kumar Lenka, Manashree Mane, Keshav.
Drafting - original draft: Rajesh Kumar Lenka, Manashree Mane, Keshav.
Writing - proofreading and editing: Rajesh Kumar Lenka, Manashree Mane, Keshav.