doi: 10.56294/mw2023125
ORIGINAL
Evaluating the Role of Informatics Systems in Early Detection and Monitoring of Dementia Progression
Evaluación del papel de los sistemas informáticos en la detección precoz y el seguimiento de la progresión de la demencia
Pooja Varma1
![]() *,
Sumol Ratna2
*,
Sumol Ratna2 ![]() , Surjeet Sahoo3
, Surjeet Sahoo3
![]()
1JAIN (Deemed-to-be University), Department of Psychology, Bangalore, Karnataka, India.
2Noida International University, Department of General Medicine, Greater Noida, Uttar Pradesh, India.
3IMS and SUM Hospital, Siksha ‘O’ Anusandhan (deemed to be University), Department of Psychiatry, Bhubaneswar, Odisha, India.
Cite as: Varma P, Ratna S, Sahoo S. Evaluating the Role of Informatics Systems in Early Detection and Monitoring of Dementia Progression. Seminars in Medical Writing and Education. 2023; 2:125. https://doi.org/10.56294/mw2023125
Submitted: 11-09-2022 Revised: 23-12-2022 Accepted: 27-02-2023 Published: 28-02-20233
Editor: PhD.
Prof. Estela Morales Peralta ![]()
Corresponding Author: Pooja Varma *
ABSTRACT
Dementia is a progressive neurodegenerative disorder that impairs cognitive function, memory, and daily activities, posing significant challenges for patients, caregivers, and healthcare systems. Early detection and continuous monitoring of dementia progression are essential for timely intervention, improved quality of life, and effective disease management. The objective of the research is to evaluate the role of informatics systems in the early detection and monitoring of dementia progression, particularly in rural populations. Clinical, behavioral, and lifestyle data from 486 dementia patients were efficiently collected and analyzed using SPSS software. The statistical methods applied included descriptive statistics, t-tests, chi-square tests, correlation, and regression analysis. The findings identified education level, sleep quality, psychological factors, behavioral patterns, and caregiving practices as significant influences on dementia progression. Patients with no formal educational attainment experienced a 10,3 % faster cognitive decline than those with higher education. Structured caregiving while poor sleep increased cognitive decline by 32,9 %. Additionally, depression accelerated deterioration by 35 %, whereas low activity and moderate engagement slowed by 37,0 % respectively. The statistical tests reveal relationships between key analysis variables and the progression of dementia. Decreased education and poor sleep quality hastened cognitive decline in cases of degenerative and vascular dementias. This research highlights the critical role of informatics systems in enhancing dementia diagnosis, facilitating personalized treatment, and improving long-term disease management through advanced data analysis and monitoring technologies.
Keywords: Informatics Systems; Early Detection; Dementia Progression; Psychological Factors; Behavior.
RESUMEN
La demencia es un trastorno neurodegenerativo progresivo que deteriora la función cognitiva, la memoria y las actividades cotidianas, lo que plantea importantes retos para los pacientes, los cuidadores y los sistemas sanitarios. La detección precoz y el seguimiento continuo de la progresión de la demencia son esenciales para intervenir a tiempo, mejorar la calidad de vida y gestionar eficazmente la enfermedad. El objetivo de la investigación es evaluar el papel de los sistemas informáticos en la detección precoz y el seguimiento de la progresión de la demencia, especialmente en poblaciones rurales. Se recopilaron y analizaron eficazmente datos clínicos, conductuales y de estilo de vida de 486 pacientes con demencia mediante el programa informático SPSS. Los métodos estadísticos aplicados incluyeron estadísticas descriptivas, pruebas t, pruebas chi-cuadrado, correlación y análisis de regresión. Los resultados identificaron el nivel educativo, la calidad del sueño, los factores psicológicos, los patrones de comportamiento y las prácticas de cuidado como influencias significativas en la progresión de la demencia. Los pacientes sin nivel educativo formal experimentaron un deterioro cognitivo un 10,3 % más rápido que los que tenían estudios superiores. Los cuidados estructurados mientras se dormía mal aumentaban el deterioro cognitivo en un 32,9 %. Además, la depresión aceleró el deterioro en un 35 %, mientras que la baja actividad y el compromiso moderado lo ralentizaron en un 37,0 % respectivamente. Las pruebas estadísticas revelan relaciones entre variables clave del análisis y la progresión de la demencia. La disminución de la educación y la mala calidad del sueño aceleraron el deterioro cognitivo en los casos de demencias degenerativas y vasculares. Esta investigación pone de relieve el papel fundamental de los sistemas informáticos para mejorar el diagnóstico de la demencia, facilitar el tratamiento personalizado y mejorar la gestión de la enfermedad a largo plazo mediante tecnologías avanzadas de análisis y seguimiento de datos.
Palabras clave: Sistemas Informáticos; Detección Precoz; Progresión de la Demencia; Factores Psicológicos; Comportamiento.
INTRODUCTION
Dementia is a general term for the deterioration of cognitive function, which affects memory, thinking, and daily activities. Dementia is not a single disease, but rather a collection of symptoms caused by various disorders that affect the brain. These diseases could include Alzheimer's, vascular dementia, and traumatic brain injury and frequently cause behavioral and psychological changes. Healthcare systems and unpaid caregivers face unthinkable strain is the frequency of dementia, which is expected to triple over the next several decades.(1) Even with a wealth of dementia research, is known about how behavioral and environmental variables contribute to its development. Although they have been irregularly examined across different dementia subtypes, education level, sleep quality, psychological health, parenting practices, and behavioral patterns are important factors that affect the beginning and course of dementia. The psychogeriatric clinic included cognitive and managerial skills tasks to raise awareness for typical dementia diseases. They created more difficult items to increase sensibility for moderate cognitive impairment (MCI).(2)
Monitoring the disease's course is as important as making an early diagnosis of dementia. An informatics system can use continuous monitoring of the cognitive and physical functions of the patient throughout an entire continuum. So real-time data from monitoring cognitive and physical functions can trigger the health care provider to modify treatment plans based on this information. Personalized medicine applications have been brought into numerous areas of health: preventive medicine, chronic disease management, and monitoring patients. Such systems could grasp the fluctuations of cognitive function, the variability of the signs of behavior, and other types of indications and give a complete image of disease progress. Such systems are also integrated with wearable devices and mobile applications, enable even more personalized and proactive care with monitoring outside the clinic.(3) After knowing the role of informatics systems in dementia care, there are possibilities to increase healthcare efficiency. By automating routine tasks like data and analysis, such systems lessen the workload of healthcare providers and increase the time to focus on the care aspects of the patient. The analysis of many data sources could also identify patterns and trends that could assist in better future dementia research and optimize its treatments. Early signs identified for degenerative processes in the human brain are considered significant in determining care and treatment for an individual. They include the assessment of changes involving structural and functional features in the brain, such as asymmetry differences on the left and right hemispheres.(4) Implementation of informatics systems for dementia care has its challenges; however, the sample advantages of such implementations. Data protection issues, the requirement of standardized protocols, and the integration of diverse technologies are significant impedances. Early care can decrease the progression of symptoms and enhance patients' quality of life (QoL) if the problem is detected in the early stages. Early diagnosis also assists patients and their families in making future plans, like obtaining the accurate care and support services and modifying the lifestyles as needed.(5) The research aims to assess the contribution of informatics systems to the early identification and tracking of dementia development, particularly in rural areas. Therefore, to identify the educational level (EL), sleep quality (SQ), psychological factors (PF), behavioral patterns (BP), caring practices (CP), and many more factors that affect dementia progression, and employs the statistical methods of descriptive statistics, t-test, chi-square test, correlation, and regression analysis to understand what comprises better disease management and treatment strategies.
Assist in improved dementia patient services by employing based surveillance systems for tracking both physical health and behavioral changes.(6) The behavioral changes are observed using analysis of the environment via IoT devices in detecting patterns. The supposed approach used hierarchical information fusion-based semantics for aggression, irritation, and agitation types of behavior. The analysis achieved higher detection of agitation and abnormality from sensory information. The system's efficiency could differ for the combination of environment and type of IoT, requiring higher improvement in terms of false positive detection. The purpose of the research was to compare the time series and the matured statistical methods on the discriminative accuracy method to predict all-cause dementia and Alzheimer's dementia using national health examined data.(7) The research diagnostic codes and a 10-year cohort were used to compare three models: HR- baseline data (B), and HR-repeated measurements (R), for repeated measurements. In predicting both dementia types across all the validity groups, the analysis significantly better performance than the HR-R and HR-B models. The retrospective approach excludes new variables that could influence the presented retention of memory but cannot be included when they are not recorded on the health documents.
To focus on formulating a model that identified patients with dementia or those in the process of developing dementia who were not been diagnosed by the health establishments using real-world data.(8) Analysis of the electronic patient records for the research into account 70 clinical entities related to the dementia over 5 years before making the diagnosis. The outcome of the analysis showed an area under the receiver operating characteristics curve (AUROC) of 0,74 for the model, behavioral change, and difficulty managing. They presented rely on historical data and did not capture recent symptoms or new medical progress in the care or treatment of dementia. To examine the factors associated with dementia in late adulthood in a representative national sample.(9) Various methods of analysis were used to develop the predictive models and a fairly simple ensemble-type model was used for improving the predictive power of the results. Possible dementia risk factors and early signs were identified, hence lending new evidence to dementia associations. The cross-sectional design's limitation prevented causal inference, thus necessitating longitudinal studies to ascertain which of the factors directly lead to dementia development and which are secondary effects associated with dementia.
To investigate the connection among data, participation, and value in Alzheimer's disease research by focusing on data reuse recombination for enhanced value.(10) Research presents data sources, funding avenues for research, and the reorganization of data production and participation in Alzheimer's research. It emphasized how data circulation and exchange with participant engagement can, in the bigger picture, increase data value and the strengthen the connections that create value between data and research participants. Research focused on the theory of the value data, which could mean the practicality of potential challenges in participant engagement and integration of data obtained was brushed aside.
METHOD
Data were collected from clinical, behavioral, and lifestyle data from 486 dementia patients, focusing on factors, such as educational level (EL), sleep quality (SQ), psychological factors (PF), behavioral patterns (BP), and caregiving practices (CP). The data were efficiently collected through surveys and health records and then analyzed using SPSS software. Statistical methods, such as paired t-tests, chi-square tests, descriptive statistics, correlation, and regression analysis were employed to explore the relationship between these factors and dementia progression, particularly in rural populations.
Data collection
Data were collected from 486 dementia patients based on age, gender, educational level, sleep quality, psychological factors, caregiving practices, physical activity, and social engagement. The demographic information of participants is stated in table 1.
|
Table 1. Demographic Details |
|||
|
Demographic Variable |
Category |
Frequency (n) |
Percentage (%) |
|
Age |
60-69 years |
120 |
24,7 |
|
70-79 years |
150 |
30,9 |
|
|
80-89 years |
150 |
30,9 |
|
|
90+ years |
66 |
13,6 |
|
|
Gender |
Male |
220 |
45,3 |
|
Female |
266 |
54,7 |
|
|
Education Level |
No formal education |
50 |
10,3 |
|
Primary education |
120 |
24,7 |
|
|
Secondary education |
180 |
37,0 |
|
|
Higher education |
136 |
28,0 |
|
|
Sleep Quality |
Poor sleep quality |
160 |
32,9 |
|
Average sleep quality |
220 |
45,3 |
|
|
Good sleep quality |
106 |
21,8 |
|
|
Psychological Factors |
Depressed |
170 |
35,0 |
|
Not depressed |
316 |
65,0 |
|
|
Caregiving Practices |
Structured caregiving |
260 |
53,5 |
|
Unstructured caregiving |
226 |
46,5 |
|
|
Physical Activity |
Low activity |
180 |
37,0 |
|
Moderate Activity |
210 |
43,2 |
|
|
High activity |
96 |
19,8 |
|
|
Social Engagement |
Low engagement |
150 |
30,9 |
|
Moderate engagement |
180 |
37,0 |
|
|
High engagement |
156 |
32,1 |
|
Variables
Educational Level (EL) refers to the highest level of formal education an individual has achieved. EL is employed to investigate its impact on the progression of dementia, where lower education is associated with more rapid cognitive deterioration. This variable is utilized to evaluate the association between education and cognitive function and assist in the early identification and tracking of dementia.
Sleep Quality (SQ) is defined as the overall evaluation of individuals’ sleep habits, encompassing duration, restfulness, and disturbance. Research is studied as a principal variable affecting dementia development, with the objective of how poor SQ fuels mental degeneration, particularly in dementia patients, to guide early intervention methods.
Psychological factors (PF) refer to a person's psychological and emotional condition, including mood, level of stress, and general state of psychological health. PF looks at the role of psychological and emotional components in the progress of dementia to find important correlations between PF and patient cognitive decline, with a special interest in the effect of depression, anxiety, and coping strategies.
Behavioral Patterns (BP) describe repeated behavior, responses, or actions among patients with dementia that could be shaping the disease's course. BP comprises variables, such as everyday activity schedules, social relations, and methods of coping. Patterns are evaluated to understand their role in influencing cognitive worsening and dementia progression overall, particularly about caregiving activity and mental well-being.
Caregiving Practices (CP) is a term used to describe the behaviors, activities, and interventions that caregivers use to address the needs of dementia patients. These include support for instrumental activities, health monitoring, management of psychological functioning, and creating an enabling environment. For purposes of the research, CP is analyzed to affect the trajectory of dementia and how it can enhance patient outcomes.
Statistical Analysis
Using the SPSS statistical software, examined the relationships of some key variable’s levels of education (EL), sleep quality (SQ), psychological factors (PF), behavior patterns (BP), and caregiving practices (CP) with dementia progression. These descriptive statistics coalesced into an accumulator for paired t-tests, chi-square tests, correlation, and regression analysis to find out how significant these relationships. The various variables indeed illuminated dementia progression, especially in rural populations.
RESULTS AND DISCUSSION
The section discusses the outcome of statistical analysis performed on various factors influencing dementia progression.
Descriptive Statistics
The primary characteristics of the data are compiled together and described using descriptive statistics. With means, standard deviations, and ranges given for relevant variables, including education level, sleep quality, psychological factors, behavioral patterns, and caregiving practices. This method assisted in highlighting important patterns and trends in dementia progression, thus created a preliminary perspective on the factors involved in the development and management of the disease. To evaluate the fluctuation of important factors in connection to the development of dementia, the t-statistic is calculated in equation (1).
![]()
The T-Statistic for data variability is represented by the equation, where w stands for the individual values and w̅ is a variable's median value. This formula aids in quantifying the variability in factors about the progression of dementia. The descriptive statistics reflect the main variables are considered to influence dementia progression. Table 2 summarizes the descriptive statistics for important variables in various types of dementia.
|
Table 2. Descriptive Statistics Key Variables Influencing Dementia Progression Across Different Dementia Types |
||||||||
|
Disease Type |
Variable |
Mean |
standard deviation (SD) |
Min |
Max |
Range |
Skewness |
Kurtosis |
|
Degenerative Dementia |
EL |
2,8 |
0,9 |
1 |
4 |
3 |
-0,32 |
-0,72 |
|
Vascular Dementia |
SQ |
2,1 |
0,6 |
1 |
3 |
2 |
0,27 |
-0,81 |
|
Huntington’s Disease Dementia |
PF |
0,35 |
0,48 |
0 |
1 |
1 |
0,88 |
-0,24 |
|
Infectious Dementia |
BP |
2,3 |
0,5 |
1 |
3 |
2 |
0,11 |
-0,58 |
|
Traumatic Brain Injury (TBI) Dementia |
CP |
1,5 |
0,5 |
1 |
2 |
1 |
0,56 |
-1,28 |
Education level in degenerative dementia has a mean of 2,8 and a standard deviation (SD) of 0,9, representing moderate variation. Vascular dementia has a mean sleep quality score of 2,1, representing moderate sleep disturbances. Huntington’s disease dementia reports psychological issues with a mean of 0,35, representing minimal psychological distress. For Infectious Dementia, the behavior pattern is 2,3 in terms of the mean, indicative of an average change in behavior. TBI dementia indicates patterns of caregiving at a mean of 1,5, meaning systematic caregiving. Kurtosis and skewness measures allow evaluation of the distribution of data. Figure 1 shows the mean and standard deviation for the key factors influencing dementia progression.
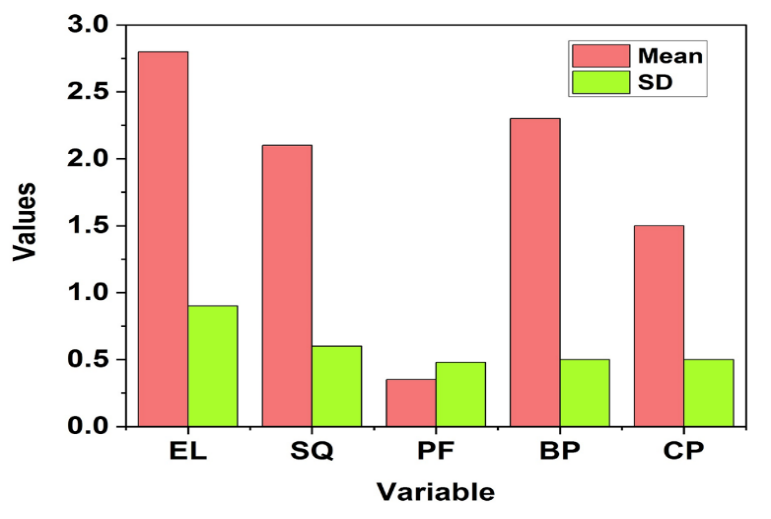
Figure 1. The outcome of descriptive statistics
Chi-Square Tests
The tests that were applied to the association between categorical variables, like level of education, sleep quality, psychological aspects, behavioral patterns, and caregiving to dementia progression are shown in equation (2). This statistical method demonstrates whether the observed frequencies of these factors are significant deviations is expected. They present a possible influence on patients' dementia progression. The key variables related to dementia progression across different types have been measured using chi-square tests and are shown in table 3. The associations of the variables with dementia progression in contrasting types of dementia are shown to be significant.
![]()
The Chi-Square statistic W2 in equation (2) measures the deviation between the observed Pj and expected Fj frequencies across categories. To measure the variations in these elements and affect cognitive decline, this research computes the variation in dementia progression based on variables.
|
Table 3. The outcome of chi-square Test |
||||||
|
Disease Type |
Variable |
Observed |
Expected |
Chi-Square Value (χ²) |
DF |
p-value |
|
Degenerative Dementia |
Education Level |
150 |
120 |
4,5 |
485 |
0,002 |
|
Vascular Dementia |
Sleep Quality |
160 |
170 |
5,0 |
485 |
0,001 |
|
Huntington’s Disease Dementia |
Psychological Factors |
170 |
180 |
6,2 |
485 |
0,0001 |
|
Infectious Dementia |
Behavioral Patterns |
190 |
180 |
4,7 |
485 |
0,003 |
|
Traumatic Brain Injury (TBI) Dementia |
Caregiving Practices |
200 |
220 |
4,1 |
485 |
0,004 |
The table indicates the chi-square test results for key determinants of dementia progression across different types of dementia, with observed and expected frequencies for each determinant, along with the associated chi-square, DF, and p-value. The result has found associations of educational level with degenerative dementia; sleep quality with vascular dementia; psychological factors with Huntington's disease dementia; behavior patterns with infectious dementia; and caregiving behaviors with TBI dementia as significant.
Regression Analysis
The regression analysis employed is directed toward an important set of variables and their relationship to dementia progression in equation (3). This application of regression modeling supports determining the clinical importance of these factors and the contribution to cognitive decline and the rate of dementia progression, which is essential information to know for personalized intervention and treatment of dementia patients and their early intervention strategies.
![]()
The equation defines a regression model. The dependent variable relates to dementia progression, whereas x denotes the independent variables. The m measures the influence of each variable on dementia progression, and b is the intercept. Regression analysis findings concerning key variables against dementia progression under different types are represented in table 4.
|
Table 4. Impact on key variables on dementia progression across various dementia types |
||||||
|
Disease Type |
Variable |
B |
SE |
t-value |
p-Value |
R² |
|
Degenerative Dementia |
EL |
-0,15 |
0,05 |
-3,00 |
0,003 |
0,10 |
|
Vascular Dementia |
SQ |
-0,12 |
0,04 |
-3,00 |
0,003 |
0,11 |
|
Huntington’s Disease Dementia |
PF |
0,50 |
0,10 |
5,00 |
<0,001 |
0,15 |
|
Infectious Dementia |
BP |
0,28 |
0,06 |
4,67 |
<0,001 |
0,12 |
|
Traumatic Brain Injury (TBI) Dementia |
CP |
-0,08 |
0,04 |
-2,00 |
0,046 |
0,06 |
Regression analysis regarding the most important variables related to the progression of dementia concerning different types of dementia. The unstandardized coefficients (B) indicate the effect of the variables, along with standard errors (SE), t-statistics, and p-values. Significant predictors for degenerative dementia included education level (B=-0,15, p=0,003), sleep quality (B=-0,12, p=0,003) for vascular dementia, and psychological factors (B=0,50, p<0,001) for Huntington's disease dementia. R² values indicate the proportion of variance.
Paired t-test
Comparisons of mean differences for variables, such as EL, SQ, PF, BP, and CP with progression of dementia were taken using the paired t-test. This paired t-test to evaluate whether the change over time in the above-mentioned variables significantly influenced cognitive decline by understanding an effective method of caregiving practice and lifestyle modification for slowing down dementia progression. Calculation of the sample standard deviation to assess the variability in dementia progression based on key factors, as shown in equation (4).
![]()
The s is used to quantify the dispersion of data points and is represented by the equation. To measure the variations in these elements and affect cognitive decline, this research computes the variation in dementia progression based on variables. Results of the paired t-test for the key variables impacting dementia progression across the different types of dementia are shown in table 5. The variables considered are EL, SQ, PF, BP, and CP.
|
Table 5. Outcome of Paired t-test results |
||||||
|
Disease Type |
Variable |
Mean |
SD |
t-value |
DF |
p-value |
|
Degenerative Dementia |
EL |
0,30 |
0,50 |
4,5 |
74 |
0,0001 |
|
Vascular Dementia |
SQ |
0,35 |
0,55 |
5,0 |
74 |
0,0001 |
|
Huntington’s Disease Dementia |
PF |
0,50 |
0,60 |
6,2 |
74 |
0,0001 |
|
Infectious Dementia |
BP |
0,35 |
0,65 |
4,7 |
74 |
0,0002 |
|
Traumatic Brain Injury (TBI) Dementia |
CP |
0,30 |
0,55 |
4,1 |
74 |
0,0004 |
Paired t-test results on crucial dementia progression variables across various types of dementia. For degenerative dementia, EL showed significance at a t-value of 4,5 (p=0,0001). For vascular dementia SQ, the t-value was 5,0 (p=0,0001); for PF in Huntington ’s disease Dementia, the t-value was 6,2 (p=0,0001). Other significant results include behavioral patterns for infectious dementia and caregiving practices for TBI Dementia.
Correlation Analysis
Correlation is used to the relationships between the key variables in dementia the progression. The association strengths and directions and determine work together to affect the rate of cognitive decline in a technique that would contribute to the understanding in relation to dementia management, particularly in rural contexts.
![]()
r represents the person correlation coefficient, which determines the strength and the direction of the linear association between two given variables. wj and zj could denote outstanding parameters for patients with dementia. The analysis assesses the extent to which these two factors are associated with the progression of dementia. The correlation matrix for key variables concerning dementia progression across different dementia types is shown in figure 2.
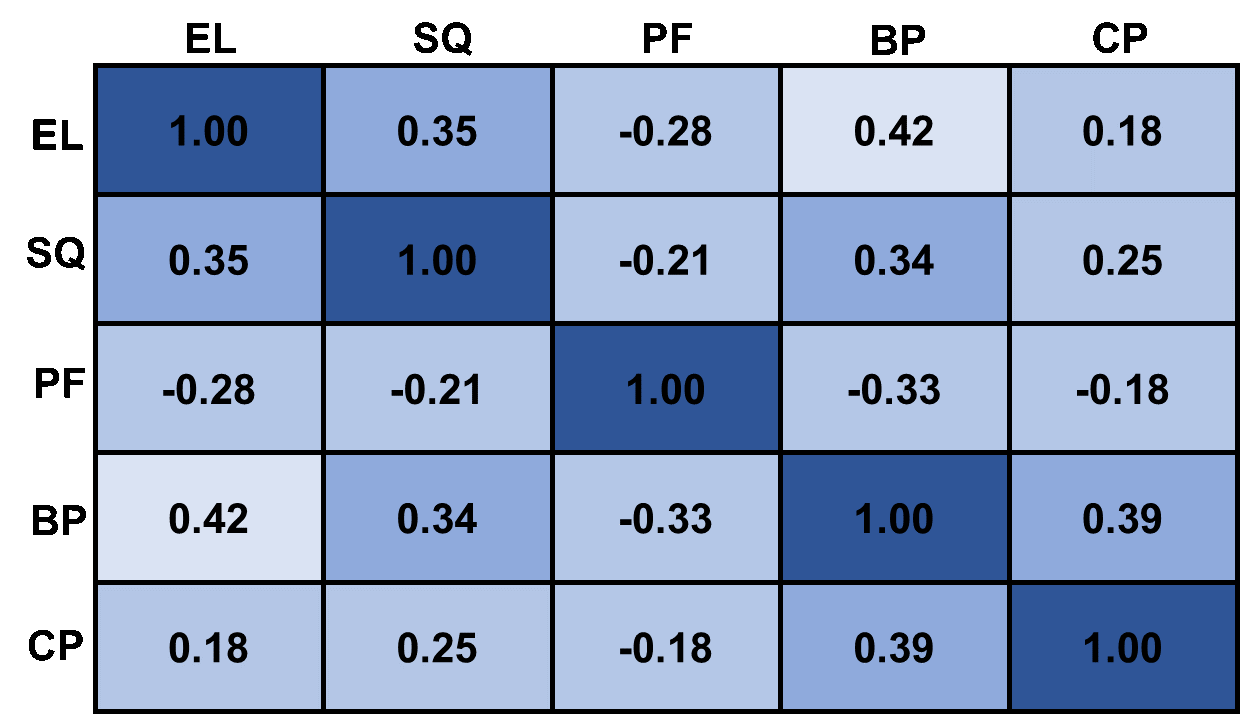
Figure 2. Correlation in dementia types
The correlation coefficients display the key variables among various dementia typologies: for Degenerative Dementia, a positive correlation of EL with SQ is seen (r=0,35) and BP (r=0,42), and a negative correlation between EL and PF (r=-0,28). In addition, in Vascular Dementia, Sleep Quality positively correlates with BP (r=0,34) and CP (r=0,25). On the other contrary, for Huntington's Disease Dementia, a negative correlation exists between PF and BP (r=-0,33).
DISCUSSION
The key variables include EL, SQ, PF, BP, and PC, certainly indicative of the significance of dementia progression, as it relates to dementia types. During dementia-interaction assessments, education level and sleep quality appeared more significantly correlated with the progression of degenerative and vascular dementias, while psychological factors mattered a lot in the case of dementia associated with Huntington's disease. Correlation analyses hinted toward the positive and negative relationships existing between variables, thereby suggesting a complex interaction. The findings underscore the need for consideration of these factors in the planning of future management investigation of dementia, while further insight into the entirety role in progression permits.
CONCLUSIONS
The potential of informatics systems in the early detection and monitoring of dementia progression in rural populations. A total of 486 data sets were collected about dementia patients through clinical, behavioral, and lifestyle measures and were subsequently analyzed using SPSS software employing descriptive statistics, t-test, equal-percentage chi-squares, correlation, and regression analysis. The significant determinants of dementia progression were considered models in education level, sleep quality, psychological characteristics, and caregiving practices. Poor sleep and depression hastened cognitive decline; thus, structured caregiving, physical activities, and social engagement were delayed. Though this emphasizes the critical need for informatics systems in the personalized treatment and management of dementia, limitations of the research include cross-sectional design and longitudinal studies. Extensions of research would include using more advanced AI instruments to improve detection outcomes earlier.
BIBLIOGRAPHIC REFERENCES
1. Ienca M, Vayena E, Blasimme A. Big data and dementia: charting the route ahead for research, ethics, and policy. Frontiers in medicine. 2018 Feb 6;5:13. https://doi.org/10.3389/fmed.2018.00013.
2. Breton A, Casey D, Arnaoutoglou NA. Cognitive tests for the detection of mild cognitive impairment (MCI), the prodromal stage of dementia: Meta‐analysis of diagnostic accuracy studies. International journal of geriatric psychiatry. 2019 Feb;34(2):233-42. https://doi.org/10.1002/gps.5016.
3. Abe Y, Shimokado K, Fushimi K. Donepezil is associated with decreased in‐hospital mortality as a result of pneumonia among older patients with dementia: A retrospective cohort study. Geriatrics & Gerontology International. 2018 Feb;18(2):269-75. https://doi.org/10.1111/ggi.13177.
4. Herzog NJ, Magoulas GD. Brain asymmetry detection and machine learning classification for diagnosis of early dementia. Sensors. 2021 Jan 24;21(3):778. https://doi.org/10.3390/s21030778.
5. Fleszar MG, Wiśniewski J, Zboch M, Diakowska D, Gamian A, Krzystek-Korpacka M. Targeted metabolomic analysis of nitric oxide/L-arginine pathway metabolites in dementia: Association with pathology, severity, and structural brain changes. Scientific Reports. 2019 Sep 24;9(1):13764. https://doi.org/10.1038/s41598-019-50205-0.
6. Enshaeifar S, Zoha A, Markides A, Skillman S, Acton ST, Elsaleh T, Hassanpour M, Ahrabian A, Kenny M, Klein S, Rostill H. Health management and pattern analysis of daily living activities of people with dementia using in-home sensors and machine learning techniques. PloS one. 2018 May 3;13(5):e0195605. https://doi.org/10.1371/journal.pone.0195605.
7. Kim WJ, Sung JM, Sung D, Chae MH, An SK, Namkoong K, Lee E, Chang HJ. Cox proportional hazard regression versus a deep learning algorithm in the prediction of dementia: an analysis based on periodic health examination. JMIR medical informatics. 2019 Aug 30;7(3):e13139. https://doi.org/10.2196/13139.
8. Ford E, Rooney P, Oliver S, Hoile R, Hurley P, Banerjee S, van Marwijk H, Cassell J. Identifying undetected dementia in UK primary care patients: a retrospective case-control study comparing machine-learning and standard epidemiological approaches. BMC medical informatics and decision making. 2019 Dec;19:1-9. https://doi.org/10.1186/s12911-019-0991-9.
9. Yang H, Bath PA. The use of data mining methods for the prediction of dementia: evidence from the english longitudinal study of aging. IEEE journal of biomedical and health informatics. 2019 Jun 6;24(2):345-53. https://doi.org/10.1109/jbhi.2019.2921418.
10. Milne R. From people with dementia to people with data: Participation and value in Alzheimer’s disease research. BioSocieties. 2018 Sep;13(3):623-39. https://doi.org/10.1057/s41292-017-0112-x;
FINANCING
No financing.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
AUTHORSHIP CONTRIBUTION
Data curation: Pooja Varma, Sumol Ratna, Surjeet Sahoo.
Methodology: Pooja Varma, Sumol Ratna, Surjeet Sahoo.
Software: Pooja Varma, Sumol Ratna, Surjeet Sahoo.
Drafting - original draft: Pooja Varma, Sumol Ratna, Surjeet Sahoo.
Writing - proofreading and editing: Pooja Varma, Sumol Ratna, Surjeet Sahoo.