doi: 10.56294/mw2023135
Original
Telemedicine-Enabled Blood Glucose Monitoring as an Effective Strategy for Reducing Hypoglycaemia Risk in Diabetes
Monitorización de la glucemia mediante telemedicina como estrategia eficaz para reducir el riesgo de hipoglucemia en la diabetes
Jaya Bhanu Kanwar1 ![]() *, Uzma Noor Shah2
*, Uzma Noor Shah2 ![]() , Sachet Dawar3
, Sachet Dawar3 ![]()
1IMS and SUM Hospital, Siksha ‘O’ Anusandhan (deemed to be University), Department of Endocrinology, Bhubaneswar, Odisha, India.
2School of Sciences, JAIN (Deemed-to-be University), Department of Genetics, Karnataka, India.
3Noida International University, Department of Medicine, Greater Noida, Uttar Pradesh, India.
Cite as: Kanwar JB, Noor Shah U, Dawar S. Telemedicine-Enabled Blood Glucose Monitoring as an Effective Strategy for Reducing Hypoglycaemia Risk in Diabetes. Seminars in Medical Writing and Education. 2023; 2:135. https://doi.org/10.56294/mw2023135
Submitted: 23-09-2022 Revised: 18-12-2022 Accepted: 26-02-2023 Published: 27-02-2023
Editor: PhD.
Prof. Estela Morales Peralta ![]()
Corresponding author: Jaya Bhanu Kanwar *
ABSTRACT
Hypoglycaemia remains an important hazard in Diabetes Mellitus (DM) management, causing severe health problems and reduced Quality of Life (QoL). Traditional monitoring systems often need the concurrent response essential to efficiently mitigate hypoglycaemic incidents. Telemedicine-enabled Blood Glucose (BG) monitoring incorporates innovative technology with remote healthcare access, offering an advanced solution for enhancing glycemic outcomes. The research evaluates the influence of telemedicine-enabled BG monitoring on reducing hypo-glycaemia risk, glycemic variability, and improving overall diabetes management effects. A total of 83 individuals with DMT1 and DMT2 are included. Participants are split into two cohorts: the intervention cohort utilized telemedicine-enabled constant glucose monitoring methods, while the control cohort employed standard monitoring techniques. The intervention included concurrent data sharing, tele-consultations, and modified suggestions. Statistical analyses incorporated regression and Analysis of Variance (ANOVA) to estimate the effects of hypoglycaemia frequency, glycated hemoglobin (HbA1c) levels, and glycemic variability. The intervention cohort established a significant decrease in hypoglycaemic incidents (p < 0,05) and enhanced glycemic constancy compared to the control cohort. HbA1c levels illustrated notable enhancement, and observance to treatment procedures superior in the telemedicine cohort. Participants also reported improved satisfaction and self-reliance in managing their diabetes. Telemedicine-enabled BG monitoring efficiently reduces hypoglycaemia threat and improves glycemic outcome, observance, and patient confidence. This system provides a hopeful pathway for recovering diabetes management and recovering QoL.
Keywords: Telemedicine; BG Monitoring; Glycated Hemoglobin (Hba1c); Digital Health Technologies; Glycemic Control.
RESUMEN
La hipoglucemia sigue siendo un riesgo importante en el tratamiento de la diabetes mellitus (DM), que causa graves problemas de salud y reduce la calidad de vida (CdV). Los sistemas de control tradicionales a menudo necesitan la respuesta simultánea esencial para mitigar de manera eficiente los incidentes de hipoglucemia. El control de la glucosa en sangre (GS) mediante telemedicina incorpora tecnología innovadora con acceso a atención médica remota, lo que ofrece una solución avanzada para mejorar los resultados glucémicos. La investigación evalúa la influencia del control de la GS mediante telemedicina en la reducción del riesgo de hipoglucemia, la variabilidad glucémica y la mejora de los efectos generales del control de la diabetes. Se incluye un total de 83 personas con DMT1 y DMT2. Los participantes se dividen en dos cohortes: la cohorte de intervención utilizó métodos de control constante de la glucosa mediante telemedicina, mientras que la cohorte de control empleó técnicas de control estándar. La intervención incluyó el intercambio simultáneo de datos, teleconsultas y sugerencias modificadas. Los análisis estadísticos incorporaron regresión y análisis de varianza (ANOVA) para estimar los efectos de la frecuencia de hipoglucemia, los niveles de hemoglobina glucosilada (HbA1c) y la variabilidad glucémica. La cohorte de intervención estableció una disminución significativa en los incidentes de hipoglucemia (p < 0,05) y mejoró la constancia glucémica en comparación con la cohorte de control. Los niveles de HbA1c ilustraron una mejora notable y la observancia de los procedimientos de tratamiento fue superior en la cohorte de telemedicina. Los participantes también informaron una mayor satisfacción y autosuficiencia en el manejo de su diabetes. El monitoreo de BG habilitado por telemedicina reduce eficazmente el riesgo de hipoglucemia y mejora el resultado glucémico, la observancia y la confianza del paciente. Este sistema proporciona una vía esperanzadora para recuperar el manejo de la diabetes y recuperar la calidad de vida.
Palabras clave: Telemedicina; Monitorización de Glucosa en Sangre; Hemoglobina Glucosilada (Hba1c); Tecnologías de Salud Digital; Control Glucémico.
INTRODUCTION
Diabetes mellitus (DM) is the most severe global non-infectious illnesses, raising a significant risk to individual wellbeing. The World Health Organization (WHO) predicts that by 2030, 366 million people will have diabetes, more than doubling the number.(1) DM is divided into two types: type 1 DM (DM T1) and type 2 DM (DMT2), with DMT2 secretarial for roughly 95 %.(1) DMT2 is defined by insulin struggle and insulin insufficiency, which result in many organ damage and consequences. T2DM issues not only cause major physical and mental health problems, shortening life expectancy, but they also impose economic costs on both individuals and society.(2)
The frequency and harshness of difficulties are mostly determined by the progression of diabetes and BG management. As a result, people with T2DM must maintain excellent metabolic control. The clinicians are primarily responsible for controlling Blood Glucose (BG) and other Biochemical markers in T2DM individuals, which is generally standardized.(3) However, outside of hospitals, diabetes patient management is chaotic, lacks consistency, and is mostly dependent on patient education and engagement. As a result, self-management and suitable managing tactics are especially significant for diabetic patients.(4) Despite data that self-monitoring of BG (SMBG) and a well routine are advantageous for illness control, implementing effectual SMBG and enduring life modifications is a significant every day struggle. The downsides of SMBG are primarily connected to individuals who lack motivation or are unaware of when to assess and how to understand the data.(5)
People with diabetes have long used technology to self-manage and increase treatment compliance. Telephone coaching, text message service maintain, and telemedicine-based methods have all been exposed to enhance executive observance and, as an effect, glycemic control.(6) The widespread use of mobiles has facilitated the growth of diabetes management applications (apps), which have emerged as important decision, and disease administration tools for both diabetics and medical professionals. The recently designed telemedicine method is a versatile incorporation of examining, counselling, and life involvement that allows for the customisation of SMBG.(7) Evaluated to traditional techniques of persistent disease organization, the remote healthcare method not only highlights the significance of individual’s self-care but also develops suitable interaction among individuals and medicinal contributors, resulting in fewer hospital visits.(8) Telemedicine is a capable method for providing individualized SMBG and medicine at residence or wherever it is required, hence decreasing the needless use of medical sources. Nevertheless, there is indeed a lack of reliable data on real scientific effect evaluation for precise diseases, like alterations in glycated hemoglobin (HbA1c) intensities in diabetes.(9) One disadvantage is the lack of understanding about the usefulness of tele-medical strategy in supporting DM care. Indication of such efficiency is having an influence on the general illness trouble by minimizing needless use of healthcare sources.(10) The research evaluated how structured SMBG with and without Tele-Care help affected glycemic control in DMT2.(11) A 12-month assessment included 446 patients and compared usual care, SMBG alone, and SMBG plus Tele-Care. SMBG significantly decreased HbA1c levels, while Tele-Care had no further benefit. Limitations included participant dropout and possible self-selection bias.
The influence of SMBG incidence on glycemic effects was assessed in the research employing a unique BGM device with real-time data transfer.(12) A subsequent analysis of a nonrandomized trial involving 359 T2DM patients found that 1,5 daily Finger Stick BG (FSBG) checks significantly decreased HbA1C. Limitations include a non-randomized design and reliance on self-monitoring of adherence.
The investigation evaluated the outcome of a digital fitness program on HbA1c and Fasting BG (FBG) levels in individuals with DMT2.(13) The experiment, including 65 patients, obtained self-reported FBG data via automated communications. The intervention dramatically lowered HbA1c and FBG, however engagement rates varied, necessitating additional modification.
This research investigated the consequence of a mobile-enabled app on glycemic control in DMT2 individuals who had begun insulin therapy. (14) Retrospective analysis revealed significant reductions in fasting and postprandial glucose levels after 12 weeks (P < 0,001). Frequent monitoring enhanced target glucose accomplishment while decreasing hypoglycaemia. Limitations included retrospective design and the possibility of selection bias.
The investigation assessed the efficiency of a culturally customized Telemonitoring method in recovering glycemic outcome in Asian T2DM patients.(15) A randomized controlled experiment with 330 participants will monitor HbA1c levels, blood pressure, and QoL over a 24-month period. The findings informed telemedicine adoption, although long-term adherence remains a challenge.
Using a cross-sectional survey of 721 participants, the analysis investigated SMBG adherence among Chinese T2DM patients and the factors that influence it.(16) Key factors discovered by multivariate research were treatment regimen, personal glucose meter ownership, and education level. Limitations include the use of self-reported data and the need for bigger, multicenter research.
This investigation compared remote Telemonitoring with team-based concern for uncontrolled DMT2.(17) Around 240 patients were evaluated throughout the course of 52 weeks utilizing home glucose monitors. The intervention resulted in small HbA1c improvements but no meaningful secondary outcome differences. The little benefit showed that further initiatives were needed to improve diabetes care involvement.
The research evaluated the effectiveness of Smartphone-based, concurrent diabetes concern.(18) For 12 weeks, forty DMT2 patients were randomly dispersed to one of two cohorts: smartphone-based (SC) or conventional therapy. SC showed superior glucose management (A1C ≤6,5 %) compared to CC (47,1 % vs 11,1 %, P = 0,019). However, a small sample size reduces generalisability.
Existing research on SMBG, Telemonitoring, and digital health interventions reveals limitations in telemedicine’s effectiveness, patient engagement, and long-term adherence. SMBG lowers HbA1c. However, Tele-Care provides no meaningful benefit. Small sample sizes and selection bias restrict generalisability. Most analyses don’t include real-time advice or behavioral reinforcement. This research addresses these gaps by combining telemedicine-enabled continuous glucose monitoring, remote consultations, and individualized feedback to enhance glycemic outcomes and adherence. The objective is to assess the influence of telemedicine-enabled BG monitoring on reducing hypoglycaemia risk, minimizing glucemic variability and enhancing overall diabetes management outcomes. The research aims to assess improvements in hypoglycaemia frequency, glycated hemoglobin levels and patients adherence compared to the standard monitoring method.
Highlights of the research
Hypoglycaemia is a key difficulty in diabetes care, often leading to severe consequences and reduced Quality of Life (QoL). Highlights of the research are given below:
· The objective is to assess how telemedicine-enabled constant glucose monitoring enhances glycemic control, reduces hypoglycaemia risk and enhances adherence to diabetes management protocols.
· The data is gathered from 83 participants with DMT1 and DMT2. Individuals are divided into intervention and control cohorts to compare telemedicine-enabled monitoring with standard method.
· The findings highlight that telemedicine improves treatment adherence, patient confidence and overall satisfaction, reinforcing its role in effective diabetes management.
Healthcare providers and policymakers should integrate telemedicine into diabetes care framework, promoting real-time monitoring and remote consultations to improve individual results, reduce difficulties and enhance QoL.
METHOD
The data is gathered from 83 individuals on demographic and health-related characteristics, with precise inclusion and exclusion criteria. Participants are separated into two cohorts: control and intervention, with hypoglycaemia frequency, glycemic variability, and HbA1c levels measured. Statistical analyses in Statistical Package for the Social Sciences (SPSS) 27 used Analysis of Variance (ANOVA) and logistic regression to assess the efficiency of interventions.
Data collection
The data is gathered from 83 participants with DMT1 and DMT2. A questionnaire was utilized for collecting demographic and health-associated data.
Selection criteria
The selection criteria ensure the significance of the sample for the investigation. There are both exclusion and inclusion measures.
Inclusion criteria
The individuals had a type 1 or type 2 diabetes diagnoses recorded in their electronic medical records (EMR) and an HbA1c level between 7 % and 10 %, indicating their most recent glycemic management. They had nil or gentle benign diabetes retinopathy lacking retinal association. Participants also had to agree to use standard observing utensils that coordinated with the Tele-monitoring method for the entire six-month research period, as specified in the protocol.
Exclusion criteria
Individuals with poorly controlled glycemic levels, defined as an HbA1c value greater than 10 %, as well as those with dementia injury, are excluded. Participants with pre-existing retinal conditions, such as moderate to severe proliferative diabetic retinopathy or other retinal and macular illnesses, are excluded. Individuals with chronic kidney disease in stages 3b, 4, or 5 were excluded, as were those with established peripheral vascular, coronary, or cerebrovascular disorders. Patients with final-stage diseases with an existence expectancy of less than two years, as well as pregnant women, are excluded.
These criteria ensured that participants had a relatively homogeneous background for assessing BG Monitoring.
Data splitting
The research evaluates postpartum care’s impact on hypoglycaemia. The data is split into two cohorts, a control, and an investigational cohort. Patients are trained to examine their BG levels, exercise, and maintain a food dietary. To prevent hypoglycemia, patients are advised to engage in aerobic, resistive, or flexible exercise at a reasonable intensity, at least three times a week, and for 150 minutes. At baseline, all patient cohorts received typical diabetes concern instruction from a healthcare professional.
Control cohort
The CC cohort did not get any comment or diabetic instruction discussion following baseline education.
Interventional cohort
TG participants are given a gluco-telemeter that regularly transmitted BG measurements to a website. They are instructed to provide up to six readings per week to a centralized attendant. During the six-month program, they received programmed response on glycemic and metabolic outcomes. If three successive measurements suggested hypoglycaemia or hyperglycemias, a communication is sent to the attending physicians or an investigator for potential medicinal adjustments based on a procedure. If 75 % of interpretations are within the 200 mg/dL intention, no medication changes are recommended; if less than 75 % reach the target, treatment intensification is recommended, with final adjustments left to the doctor’s discretion. If there are any side effects, clinicians would adjust the dosage. The individuals also got periodical communications on self-supervision, glucose control, and medicine observance, as well as clinic visits at weeks 4, 12, and 24 for further diabetes self-executive training. From months 7 to 12, all individuals resumed their regular clinic vacations every three months or as needed but no longer received research-related assistance.
Variables
Changes in glycemic control are measured by assessing various markers, including hypoglycaemia frequency, glycemic variability, and HbA1c level at baseline and weeks 4, 8, and 12 of the care intervention.
Hypoglycaemia Frequency
The number of hypoglycaemia episodes (low BG occurrences) reported by participants was recorded. The occurrence of hypoglycaemia in patients using the telemedicine platform decreased steadily. The incidences of hypoglycaemia at baseline and weeks 4, 8, and 12 are assessed.
Glycemic Variability
BG levels are fluctuating over time, as measured by the mean or frequency of variation.
HbA1c Levels
Glycated hemoglobin (HbA1c) is an indicator that measures average levels of BG over the preceding 2-3 months. HbA1c suggests improved long-term glycemic control.
Statistical analysis
The statistics are evaluated using IBM SPSS 27 software. The data is analysed using various testes, including Descriptive statistics, ANOVA and regression analysis. Descriptive statistics are utilized to differentiate participants’ baseline characteristics in both cohorts. ANOVA is employed to evaluate hypoglycaemia frequency, glycemic variability, and HbA1c levels between cohorts. The linear regression is utilized to evaluate the intervention’s effect on glycemic response to adjust for probable variables. This comprehensive methodology ensured a thorough assessment of the program’s efficiency in diabetes treatment.
RESULTS
The research provides an inclusive evaluation of the impact of telemedicine-enabled BG monitoring on diabetes treatment. The BG monitoring is evaluated using key variables, which include hypoglycaemia frequency, glycemic variability, and HbA1c levels. The data is evaluated utilizing ANOVA and logistic regression analysis. The demographic features of the individuals are examined to validate that the baseline settings are balanced among the investigational and control cohorts. The demographics and clinical characteristics of the investigational and control cohorts are nearly identical.
Demographic analysis
A demographic analysis is a structured display of the major features and data of the research population, categorizing them with features. Significant factors like age, BMI, type of diabetes, and Diabetes-related complication are evaluated between the investigational cohort (n = 41) and the control cohort (n = 42). Table 1 and figure 1 demonstrate the traits of individuals.
|
Table 1. Demographic analysis |
|||
|
Characteristics |
Number of individuals (n=83) |
||
|
Investigational cohort (n=41) |
Control cohort (n=42) |
||
|
Age |
18-37 |
11 |
12 |
|
38-57 |
13 |
19 |
|
|
57 & above |
17 |
11 |
|
|
Gender |
Male |
25 |
23 |
|
Female |
16 |
19 |
|
|
Education level |
> secondary school |
9 |
8 |
|
Undergraduate |
22 |
19 |
|
|
Postgraduate |
10 |
15 |
|
|
Duration of diabetes |
1 to 10 |
24 |
22 |
|
Above 10 years |
17 |
20 |
|
|
Employment status |
Private |
15 |
16 |
|
Government |
13 |
12 |
|
|
Business |
4 |
8 |
|
|
Other |
9 |
6 |
|
|
No. of oral hypoglycemic agents (%) |
1 to 2 |
22 |
25 |
|
≥ 3 |
19 |
17 |
|
|
No of antihypertensive drugs (%) |
1 to 2 |
23 |
19 |
|
≥ 3 |
18 |
23 |
|
|
Type of diabetes |
DMT1 |
22 |
16 |
|
DMT2 |
19 |
26 |
|
|
BMI |
<18,5 |
7 |
3 |
|
18,5 to 24,0 |
14 |
16 |
|
|
24,0 to 28,0 |
12 |
14 |
|
|
≥ 28,0 |
8 |
9 |
|
|
Family history of T2DM |
Unknown |
11 |
7 |
|
Yes |
22 |
24 |
|
|
No |
8 |
11 |
|
|
Diabetes-related complications |
Yes |
23 |
25 |
|
No |
18 |
17 |
|
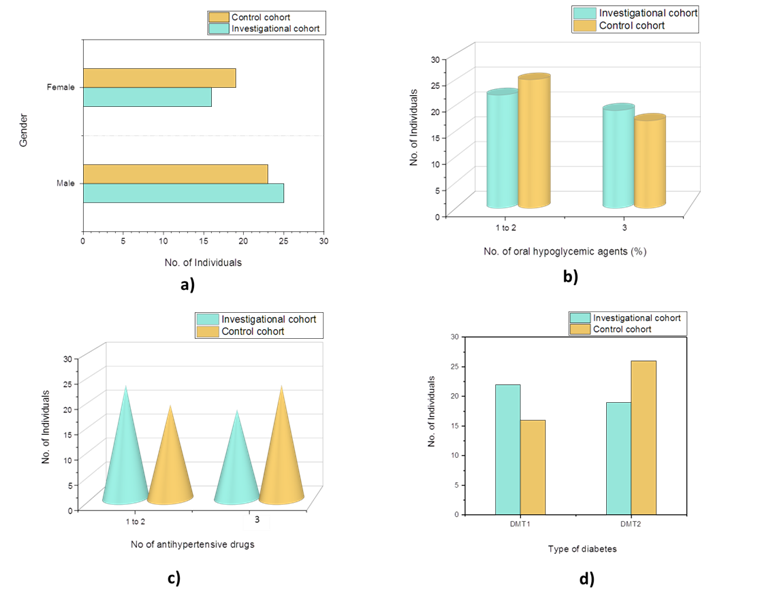
Figure 1. Representation of demographic traits
The experimental cohort comprised older patients (≥57 years, 17) and DMT1 cases,(12) whereas the control cohort had more DMT2.(16) Gender, education, employment, BMI, and diabetes-related comorbidities are all balanced to ensure comparable results. This distribution allows for a reliable assessment of the intervention’s impact on diabetes management outcomes.
Variation analysis
It evaluates the variance of two or more cohorts to see if there are any differences that are statistically significant or not. ANOVA is used to observe the differences in hypoglycemia frequency, glycemic variability, and HbA1c levels linking the investigational cohort and the control cohort. Total variation in the data is represented by the sum of square (SS), where variation within each cohort is represented by the within cohorts SS and variance between cohorts by the between cohorts SS. Table 2 and figure 2 show the statistical analysis of the features.
|
Table 2. Statistical analysis |
|||||
|
Variables |
SS |
df |
MS |
P -value |
F-value |
|
Hypoglycemia Frequency |
12,45 |
1 |
12,45 |
0,003 |
5,87 |
|
Glycemic Variability |
18,32 |
1 |
18,32 |
0,001 |
7,42 |
|
HbA1c Levels |
25,76 |
1 |
25,76 |
0,0005 |
9,63 |
|
Within cohort |
112,68 |
81 |
1,39 |
|
|
|
Between-cohort |
56,53 |
2 |
28,26 |
|
|
|
Total |
169,21 |
83 |
|
|
|
Df- degree of freedom, MS- mean square, SS-sum of square
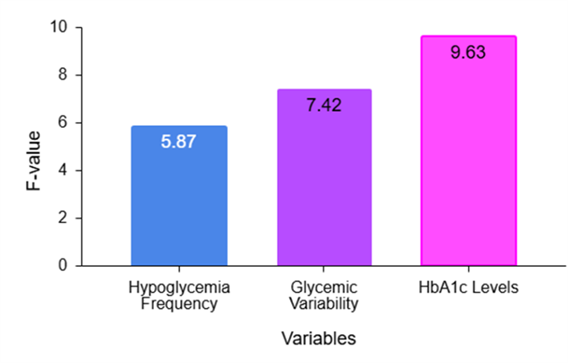
Figure 2. Analysis of F-Value
The findings show that telemedicine-enabled BG monitoring significantly improves diabetes management by lowering hypoglycaemia frequency (F = 5,87, p = 0,003) and glycemic variability (F = 7,42, p = 0,001), resulting in improved glucose stability. The biggest significant improvement is in HbA1c levels (F = 9,63, p = 0,0005), indicating better long-term management. The intervention’s effectiveness is supported by its increased between-cohort variance (MS = 28,26) over within-cohort variation (MS = 1,39), which makes it a promising method for improving diabetes self-management and QoL.
Logistic regression
Logistic regression is employed to evaluate the probability of a dual result supported on one or more analyst variables. It is employed to measure the probability of individuals in the intervention and control cohorts, supporting in influencing the efficiency of telemedicine-enabled BG monitoring in improving diabetes administration. Table 3 demonstrates the regression analysis of the variables.
|
Table 3. Regression analysis |
|||||
|
Predictor |
Cohort |
Coefficient |
Standard error |
t-value |
p-value |
|
Hypoglycemia Frequency |
Intervention |
-0,85 |
0,42 |
-4,40 |
<0,001 |
|
Control |
-0,50 |
0,38 |
-1,32 |
0,189 |
|
|
Glycemic Variability |
Intervention |
-0,92 |
0,31 |
-2,97 |
0,004 |
|
Control |
-0,30 |
0,28 |
-0,07 |
0,287 |
|
|
HbA1c Levels |
Intervention |
-0,75 |
0,18 |
-4,17 |
<0,001 |
|
Control |
-0,20 |
0,15 |
-1,33 |
0,186 |
|
The intervention cohort utilizing telemedicine-enabled BG monitoring exposed an important decrease in hypoglycaemia frequency (β = -0,85), glycemic variability (β = -0,92), and HbA1c levels (β = -0,75) when compared to the control cohort. In evaluation, the control cohort did not demonstrate statistically considerable enhancements in these variables (p > 0,05). This outcome demonstrates that telemedicine-enabled monitoring is an effectual system for recovering glycemic effect and reducing hypoglycaemia hazard in diabetes concern.
DISCUSSION
This research evaluated the effects of telemedicine-enabled BG monitoring on hypoglycaemia risk reduction, glycemic variability, and diabetes management outcomes. The demographic analysis revealed comparable baseline characteristics, with a higher proportion of elderly patients (≥57 years, 17) and DMT1 cases,(12) while the control cohort had more DMT2 cases.(16) ANOVA results showed a significant reduction in hypoglycaemia frequency (F = 5,87, p = 0,003), glycemic variability (F = 7,42, p = 0,001), and HbA1c levels (F = 9,63, p = 0,0005) in the intervention cohort, with a higher between-cohort variance (MS = 28,26), indicating its efficiency. The intervention cohort experienced significant reductions in hypoglycaemia frequency (-0,85), glycemic variability (-0,92), and HbA1c levels (-0,75), while the control cohort did not exhibit significant benefits (p > 0,05). These findings demonstrate the efficacy of telemedicine-enabled BG monitoring in improving glycemic control, increasing adherence, and boosting patient confidence, making it a promising strategy to optimize diabetes care and improve QoL.
CONCLUSION
Telemedicine-enabled BG monitoring offers a disruptive approach to diabetes treatment by combining real-time data sharing, remote consultations, and individualized recommendations to improve glycemic control and reduce hypoglycaemia risk. The research objective was to compare its effectiveness to routine monitoring in terms of reducing hypoglycaemia frequency, glycemic fluctuation, and improving overall diabetes management. The research found a substantial reduction in hypoglycaemia frequency (F = 5,87, p = 0,003), glycemic variability (F = 7,42, p = 0,001), and HbA1c levels (F = 9,63, p = 0,0005). Regression analysis also confirmed improved glycemic control (β = -0,85, p < 0,001) and higher treatment adherence. Patients reported feeling more confident and satisfied with their self-management. However, limitations include a small sample size, potential biases due to technology literacy, and the absence of long-term complication evaluation. Future research should evaluate larger, more diverse populations and evaluate long-term impacts, incorporating AI-driven predictive analytics to improve diabetes control and establishing telemedicine as a crucial tool for tailored care
REFERENCES
1. Sheemar A, Soni D, Takkar B, Basu S, Venkatesh P. Inflammatory mediators in diabetic retinopathy: Deriving clinicopathological correlations for potential targeted therapy. Indian Journal of Ophthalmology. 2021 Nov 1;69(11):3035-49. https://doi.org/10.4103/ijo.IJO_1326_21
2. Castillo‐Reinado K, Maier W, Holle R, Stahl‐Pehe A, Baechle C, Kuss O, Hermann J, Holl RW, Rosenbauer J. Associations of area deprivation and urban/rural traits with the incidence of type 1 diabetes: analysis at the municipality level in North Rhine‐Westphalia, Germany. Diabetic Medicine. 2020 Dec;37(12):2089-97. https://doi.org/10.1111/dme.14258
3. Sia HK, Kor CT, Tu ST, Liao PY, Wang JY. Self-monitoring of blood glucose in association with glycemic control in newly diagnosed non-insulin-treated diabetes patients: a retrospective cohort study. Scientific Reports. 2021 Jan 13;11(1):1176. https://doi.org/10.1038/s41598-021-81024-x
4. Jankowska-Polańska B, Świątoniowska-Lonc N, Karniej P, Polański J, Tański W, Grochans E. Influential factors in adherence to the therapeutic regime in patients with type 2 diabetes and hypertension. Diabetes research and clinical practice. 2021 Mar 1;173:108693. https://doi.org/10.1016/j.diabres.2021.108693
5. Reach G, Pellan M, Crine A, Touboul C, Ciocca A, Djoudi Y. Holistic psychosocial determinants of adherence to medication in people with type 2 diabetes. Diabetes & metabolism. 2018 Dec 1;44(6):500-7. https://doi.org/10.1016/j.diabet.2018.06.001
6. Guerci B, Chanan N, Kaur S, Jasso-Mosqueda JG, Lew E. Lack of treatment persistence and treatment nonadherence as barriers to glycaemic control in patients with type 2 diabetes. Diabetes Therapy. 2019 Apr;10(2):437-49. https://doi.org/10.1007/s13300-019-0590-x
7. Pereira MG, Pedras S, Ferreira G, Machado JC. Differences, predictors, and moderators of therapeutic adherence in patients recently diagnosed with type 2 diabetes. Journal of Health Psychology. 2020 Oct;25(12):1871-81. https://doi.org/10.1177/1359105318780505
8. Signal V, McLeod M, Stanley J, Stairmand J, Sukumaran N, Thompson DM, Henderson K, Davies C, Krebs J, Dowell A, Grainger R. A Mobile-and web-based health intervention program for diabetes and prediabetes self-management (BetaMe/Melon): process evaluation following a randomized controlled trial. Journal of Medical Internet Research. 2020 Dec 1;22(12):e19150. https://doi.org/10.2196/19150
9. Hatcher-Martin JM, Adams JL, Anderson ER, Bove R, Burrus TM, Chehrenama M, Dolan O’Brien M, Eliashiv DS, Erten-Lyons D, Giesser BS, Moo LR. Telemedicine in neurology: telemedicine work group of the American Academy of Neurology update. Neurology. 2020 Jan 7;94(1):30-8. https://doi.org/10.1212/WNL.0000000000008708
10. Staite E, Bayley A, Al-Ozairi E, Stewart K, Hopkins D, Rundle J, Basudev N, Mohamedali Z, Ismail K. A wearable technology delivering a web-based diabetes prevention program to people at high risk of type 2 diabetes: randomized controlled trial. JMIR mHealth and uHealth. 2020 Jul 15;8(7):e15448. https://doi.org/10.2196/15448
11. Parsons SN, Luzio SD, Harvey JN, Bain SC, Cheung WY, Watkins A, Owens DR. Effect of structured self‐monitoring of blood glucose, with and without additional TeleCare support, on overall glycaemic control in non‐insulin treated Type 2 diabetes: the SMBG Study, a 12‐month randomized controlled trial. Diabetic Medicine. 2019 May;36(5):578-90. https://doi.org/10.1111/dme.13899
12. Montero AR, Toro-Tobon D, Gann K, Nassar CM, Youssef GA, Magee MF. Implications of remote monitoring Technology in Optimizing Traditional Self-Monitoring of blood glucose in adults with T2DM in primary care. BMC endocrine disorders. 2021 Dec;21:1-8. https://doi.org/10.1186/s12902-021-00884-6
13. Xu R, Xing M, Javaherian K, Peters R, Ross W, Bernal-Mizrachi C. Improving HbA1c with glucose self-monitoring in diabetic patients with EpxDiabetes, a phone call and text message-based telemedicine platform: a randomized controlled trial. Telemedicine and e-Health. 2020 Jun 1;26(6):784-93. https://doi.org/10.1089/tmj.2019.0035
14. Lin J, Li X, Jiang S, Ma X, Yang Y, Zhou Z. Utilizing Technology‐Enabled Intervention to Improve Blood Glucose Self‐Management Outcome in Type 2 Diabetic Patients Initiated on Insulin Therapy: A Retrospective Real‐World Study. International Journal of Endocrinology. 2020;2020(1):7249782. https://doi.org/10.1155/2020/7249782
15. Goh KL, Lee CS, Koh CH, Ling NL, Ang SB, Oh C, Lin Y, Yuan W, Zheng QC, Tan NC. Evaluating the effectiveness and utility of a novel culturally-adapted telemonitoring system in improving the glycaemic control of Asians with type-2 diabetes mellitus: a mixed method study protocol. Trials. 2021 Dec;22:1-0. https://doi.org/10.1186/s13063-021-05240-6
16. Wang X, Luo JF, Qi L, Long Q, Guo J, Wang HH. Adherence to self-monitoring of blood glucose in Chinese patients with type 2 diabetes: current status and influential factors based on electronic questionnaires. Patient Preference and Adherence. 2019 Jul 25:1269-82. https://doi.org/10.2147/PPA.S211668
17. Lee JY, Chan CK, Chua SS, Ng CJ, Paraidathathu T, Lee KK, Lee SW. Telemonitoring and team-based management of glycemic control on people with type 2 diabetes: a cluster-randomized controlled trial. Journal of general internal medicine. 2020 Jan;35:87-94. https://doi.org/10.1007/s11606-019-05316-9
18. Ku EJ, Park JI, Jeon HJ, Oh T, Choi HJ. Clinical efficacy and plausibility of a smartphone‐based integrated online real‐time diabetes care system via glucose and diet data management: a pilot study. Internal medicine journal. 2020 Dec;50(12):1524-32. https://doi.org/10.1111/imj.14738
FINANCING
None.
CONFLICT OF INTEREST
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
AUTHORSHIP CONTRIBUTION
Conceptualization: Jaya Bhanu Kanwar, Uzma Noor Shah, Sachet Dawar.
Data curation: Jaya Bhanu Kanwar, Uzma Noor Shah, Sachet Dawar.
Formal analysis: Jaya Bhanu Kanwar, Uzma Noor Shah, Sachet Dawar.
Research: Jaya Bhanu Kanwar, Uzma Noor Shah, Sachet Dawar.
Methodology: Jaya Bhanu Kanwar, Uzma Noor Shah, Sachet Dawar.
Project management: Jaya Bhanu Kanwar, Uzma Noor Shah, Sachet Dawar.
Resources: Jaya Bhanu Kanwar, Uzma Noor Shah, Sachet Dawar.
Software: Jaya Bhanu Kanwar, Uzma Noor Shah, Sachet Dawar.
Supervision: Jaya Bhanu Kanwar, Uzma Noor Shah, Sachet Dawar.
Validation: Jaya Bhanu Kanwar, Uzma Noor Shah, Sachet Dawar.
Display: Jaya Bhanu Kanwar, Uzma Noor Shah, Sachet Dawar.
Drafting - original draft: Jaya Bhanu Kanwar, Uzma Noor Shah, Sachet Dawar.
Writing: Jaya Bhanu Kanwar, Uzma Noor Shah, Sachet Dawar.