doi: 10.56294/mw2023142
Original
Exploring Health Professionals’ Perspectives on Patient Confidentiality and Contributing Factors in Resource-Limited Environments
Exploración de las perspectivas de los profesionales de la salud sobre la confidencialidad del paciente y los factores que contribuyen a ella en entornos con recursos limitados
Ved Vrat Verma1 ![]() *, Samir Samal2
*, Samir Samal2 ![]() , RenukaJyothi S3
, RenukaJyothi S3 ![]()
1Noida International University, Department of Biotechnology, Greater Noida, Uttar Pradesh, India.
2IMS and SUM Hospital, Siksha ‘O’ Anusandhan (deemed to be University), Department of Critical Care Medicine, Bhubaneswar, Odisha, India.
3JAIN (Deemed-to-be University), Department of Biotechnology and Genetics, Bangalore, Karnataka, India.
Cite as: Verma VV, Samal S, Renuka JS. Exploring Health Professionals’ Perspectives on Patient Confidentiality and Contributing Factors in Resource-Limited Environments. Seminars in Medical Writing and Education. 2023; 2:142. https://doi.org/10.56294/mw2023142
Submitted: 01-10-2022 Revised: 03-01-2023 Accepted: 14-04-2023 Published: 15-04-2023
Editor: PhD.
Prof. Estela Morales Peralta ![]()
Corresponding author: Ved Vrat Verma *
ABSTRACT
Patient confidentiality is a fundamental ethical and legal obligation for healthcare professionals and a critical component of high-quality patient care. However, maintaining confidentiality in resource-limited environments presents significant challenges. This research explores health professionals’ perspectives on patient confidentiality and the factors influencing their knowledge, awareness, and behaviors in such settings. 323 health professionals participated, using an organized, individually conducted questionnaire established on expert validation and appropriate influencing factors. The research examined socio-demographic, work-related, and institutional factors that can impact health professionals’ perspectives on patient confidentiality. The data was analyzed using SPSS 25.0, employing descriptive statistics, t-tests, and regression analysis to assess the relationships between variables. The results indicate that only 29,5 % of participants exhibited positive behaviors toward patient confidentiality, while 42,2 % demonstrated good knowledge, and 30,3 % were aware of confidentiality principles. The findings reveal that while healthcare professionals possess a reasonable understanding of patient confidentiality, their behavioral adherence remains limited. Strengthening training programs, institutional policies and ethical awareness initiatives is crucial to enhancing healthcare professionals’ knowledge and behaviors, ultimately fostering patient trust, legal compliance, and improved healthcare quality in resource-limited environments.
Keywords: Health Professionals; Patient Confidentiality; Knowledge; Awareness; Contributing Factors.
RESUMEN
La confidencialidad del paciente es una obligación ética y legal fundamental para los profesionales de la salud y un componente crítico de la atención al paciente de alta calidad. Sin embargo, mantener la confidencialidad en entornos con recursos limitados presenta desafíos significativos. Esta investigación explora las perspectivas de los profesionales de la salud sobre la confidencialidad del paciente y los factores que influyen en su conocimiento, conciencia y comportamientos en dichos entornos. Participaron 323 profesionales de la salud, utilizando un cuestionario organizado, realizado individualmente y establecido sobre la validación de expertos y los factores de influencia apropiados. La investigación examinó los factores sociodemográficos, laborales e institucionales que pueden afectar las perspectivas de los profesionales de la salud sobre la confidencialidad del paciente. Los datos se analizaron utilizando SPSS 25.0, empleando estadísticas descriptivas, pruebas t y análisis de regresión para evaluar las relaciones entre las variables. Los resultados indican que solo el 29,5 % de los participantes exhibieron comportamientos positivos hacia la confidencialidad del paciente, mientras que el 42,2 % demostró un buen conocimiento y el 30,3 % conocía los principios de confidencialidad. Los resultados revelan que, si bien los profesionales de la salud poseen un conocimiento razonable de la confidencialidad del paciente, su adherencia conductual sigue siendo limitada. El fortalecimiento de los programas de capacitación, las políticas institucionales y las iniciativas de concienciación ética es crucial para mejorar el conocimiento y las conductas de los profesionales de la salud, fomentando en última instancia la confianza del paciente, el cumplimiento legal y una mejor calidad de la atención médica en entornos con recursos limitados.
Palabras clave: Profesionales de la Salud; Confidencialidad del Paciente; Conocimiento; Conciencia; Factores Contribuyentes.
INTRODUCTION
Patient care fundamentally depends on confidentiality, which protects health information and ensures that medical staff disclose it only in specific situations without the patient’s consent. Through confidentiality practices, medical institutions protect patient data while enabling persons to obtain treatment free from public or patient-to-patient disclosure.(1) The challenge to maintain patient confidentiality intensifies in healthcare facilities that lack both infrastructure and technological capabilities alongside minimal staff capacities.(2) Certain health facilities within low-resource areas lack protective systems for patient file management, so unauthorized personnel could access patient records. Such health care environments continue to use paper documentation, but this method exposes recorded data to high risks of damage and unauthorized use, including theft and accidental information leaks.(3) The high number of patients in medical facilities that practice shared consultations results in reduced patient privacy since their private medical discussions become easily accessible to others. Healthcare professionals face confusion regarding suitable procedures for patient data privacy because they lack training for data protection together with ethical issues.(4) Patient privacy violations occur because healthcare facilities either lack basic cybersecurity elements together with Electronic Health Records (EHRs) or do not have sufficient technological infrastructure. Staff security risks increase even when digital systems are in place due to insufficient user authorization systems, weak access restrictions and inadequate data encryption methods.(5) Digital records face a security risk due to unstable power supply and unstable internet connections; thus, health workers need to resort to non-secure platforms.(6)
When healthcare institutions face a shortage of human resources, it strongly contributes to unauthorized disclosure of confidential information. Medical staff who work under excessive workload conditions could unintentionally reveal sensitive patient information during impatient discussions.(7) A lack of well-defined policies combined with insufficient enforcement systems creates a situation where it is problematic to properly handle confidentiality breaches. The maintenance of confidentiality faces difficulties because of informal practices that exist between healthcare professionals as well as within local communities.(8)
The healthcare staff responses to organizational leadership and patient safety climate and security conditions within the workplace were assessed in this analysis. The questionnaire results demonstrate that healthcare professionals have divergent opinions compared to other staff members, thereby emphasizing the critical importance of this aspect for better medical safety.(9)
Medical workers employed at the healthy pregnancy service with an integrated antenatal clinic received an assessment to evaluate the factors that enables or restricts them from sharing lifestyle change recommendations. The research outcomes will enable better implementation of service models that embed healthy habits into prenatal care services for obese women.(10)
Research investigated the problems faced when healthcare professionals support each other in resource-limited settings. Workplace dynamics together with staff attitudes need to function, as the central component of Continuing Interprofessional Education (CIPE) programs, according to the research findings. The research presents the multiple enhancement suggestions for CIPE program planning in resource-limited settings.(11) The qualitative research evaluated Blockchain-Based Health Information Exchange (HIE) viewpoints while assessing patient and health professional and IT programmer understanding of the network.(12)
Research developed an analytical framework to determine how privacy security together with distinct personal elements, impacts Electronic Medical Record (EMR) adoption and utilization. The medical experts evaluated various perspectives before recommending this structure as their final recommendation.(13)
Research examined patients together with healthcare professional’s perspectives about the barriers diabetic patients encounter during self-care practice. The research revealed patient self-perceptions about diabetes which led to incorrect beliefs about the condition, deliberate noncompliance and the use of herbal remedies with breakage of old habits and no exercise motivation being observed as behavioral obstacles.(14)
Researchers conduct studies about consumer reactions when using blockchain-enabled HIE platforms and their potential adoption of this technology. This research produces findings about blockchain-based HIE deficiencies that medical facilities need to handle, which both scholars and practitioners will find significant.(15)
Medical professionals need to understand the strategies proposed in this research for developing Interprofessional Collaborative Practice (IPCP). The primary pillar enabling is the physical and emotional bonds that develop among healthcare workers.(16)
Research examined how medical staff working with Sensor-Based Networks (SBN) monitor chronic patients remotely through continuous tracking systems. The research showed positive views toward SBN although it exposed concerns about its effects on patient care and healthcare visits together with data confidentiality and costs.(17)
The aim of this research is to understand the healthcare staff’s perspectives on patient confidentiality management when resources are limited. It assesses healthcare workers understanding of confidentiality standards along with their conscious steps and existing knowledge. The research uncovered key elements that affect confidentiality requirements through institutional factors as well as professional characteristics and sociodemographic factors. It establishes that training programs lead to better ethical compliance performance.
METHOD
This research evaluated healthcare professionals’ views on patient confidentiality through a structured questionnaire that collected information about institutional factors with professional backgrounds and sociodemographic characteristics. Healthcare professionals underwent training on confidentiality principles followed by a pre-test evaluation to ensure questionnaire accuracy. They received the post-test four weeks later.
Data Collection
A structured self-administered questionnaire served as the instrument to collect information about healthcare professionals’ understanding of patient confidentiality issues. Table 1 depicts the demographic data. Research examined several important variables regarding gender, age, experience, occupational groups (doctor, nurse, pharmacist, or other), and workplace settings (public hospital, private hospital, or community clinic) together with institutional training on confidentiality. The knowledge levels and actions of healthcare professionals regarding patient confidentiality depend on various influencing elements. Mostly dependent on training is the fulfillment of law and ethical standards. Through this approach, researchers acquire an extensive understanding of confidentiality issues that exist in situations of restricted resources. The systematic approach enables validity as well as consistency and dependability when analyzing variables that affect confidentiality practices.
|
Table 1. Socio-Demographic and Professional Characteristics of Participants |
|||
|
Variable |
Category |
Frequency (n = 323) |
Percentage (%) |
|
Gender |
Male |
145 |
44,9 |
|
Female |
178 |
55,1 |
|
|
Age Group (years) |
20–30 |
95 |
29,4 |
|
31–40 |
110 |
34,1 |
|
|
41–50 |
72 |
22,3 |
|
|
>50 |
46 |
14,2 |
|
|
Profession |
Doctor |
102 |
31,6 |
|
Nurse |
134 |
41,5 |
|
|
Pharmacist |
45 |
13,9 |
|
|
Other |
42 |
13,0 |
|
|
Years of Experience |
<5 years |
112 |
34,7 |
|
5–10 years |
125 |
38,7 |
|
|
>10 years |
86 |
26,6 |
|
|
Work Setting |
Public Hospital |
170 |
52,6 |
|
Private Hospital |
98 |
30,3 |
|
|
Community Clinic |
55 |
17,1 |
|
|
Confidentiality Training Received |
Yes |
142 |
44,0 |
|
No |
181 |
56,0 |
|
Selection Criteria
The criteria define the characteristics qualify individuals for participation and disqualification during research studies. A precise definition of criteria helps researchers maintain validity and reliability for the investigation of relevant participants. Table 2 presents the specified participant selection requirements.
|
Table 2. Selection Criteria Process: Inclusion and Exclusion |
|
|
Inclusion Criteria |
Exclusion Criteria |
|
· Healthcare professionals are actively engaged in patient care. · Minimum of one year of professional experience. · Employed in a healthcare facility (e.g., hospitals, clinics, or community health centers). · Willing to provide informed consent for participation. · Available to complete both pre-and post-test assessments. |
· Administrative or non-clinical staff with no direct patient interaction. · Healthcare professionals with less than one year of experience. · Individuals who declined to participate or did not provide informed consent. · Participants are unable to complete both pre-and post-test assessments. · Professionals currently undergoingdisciplinary actions related toconfidentiality breaches. |
Questionnaire Conduction
The knowledge, perception, and practice related to patient privacy, sociodemographic, workplace, and organizational variables were evaluated in this research. To enhance reach, the questionnaire was developed in both paper-based and online-based versions. Each participant was allowed 20-30 minutes to fill it in separately and confidentially. The patients were assured of the confidentiality of the information and the survey was conducted voluntarily.
Pre- and Post-Test Evaluation
Pre-test: to examine the questionnaire’s reliability and intelligibility, 30 randomly chosen medical experts participated in a pre-test. Response ease, language, and question structure were all evaluated by the participants. Small changes were made to enhance flow and clarity. The anticipated time of completion was also established by the pre-test. The final questionnaire was guaranteed to be understandable and useful due to this process.
Post-test: an intervention session on patient confidentiality principles was held following the initial survey. It addressed optimal practices in environments with limited resources, case studies of violations, and ethical and legal considerations. The post-test was provided with four weeks’ notice. To assess changes, participants filled out the same questionnaire again.
Statistical Analysis
Using SPSS 25.0, the gathered data was examined, and descriptive statistics were used to highlight important factors and demographic traits. To assess the effect of the intervention on patient confidentiality-related knowledge, awareness, and behaviors, paired t-tests were used to compare pre-and post-test results. The research employed regression analysis to discover which factors primarily influenced secrecy adherence when analyzing both institutional elements and work-related and socio-demographic aspects. Research results included confidence ranges in appropriate sections of the analysis while p < 0,05 defined the statistical significance threshold. The research generated detailed information about healthcare personnel’s understanding and practice of strict patient information protection within the contexts of reduced healthcare resources.
RESULTS AND DISCUSSION
The research results demonstrate substantial inadequacies in healthcare worker’s understanding and practice of patient confidentiality protocols, impacting their ethical conduct. Training interventions displayed improvements because they demonstrated the value of structured educational programs. Healthcare institutions together with their clinical experience, play a crucial role in strengthening confidentiality procedures within medical facilities.
A descriptive analysis of the training and knowledge of healthcare professionals
The research discloses crucial information about how healthcare professionals understand patient confidentiality and their training experience along with their work environments, awareness and behavioral patterns. The research showed that positive behaviors for patient confidentiality maintenance existed in 29,5 % of participants, yet knowledge level reached 42,2 % and awareness reached 30,3 % were illustrated in table 3. The current understanding and practice of confidentiality standards remain absent at a concerning level because it puts patient trust and ethical medical practice at risk. A significant 44 % of respondents received formal training about confidentiality but 56 % not received such training, which shows a necessity for established training programs. Different healthcare facilities served as employment bases, including 52,6 % in public hospitals versus 30,3 % in private facilities and 17,1 % in community clinics, thus indicating varying confidentiality practices by institution. Among the sample participants, 34,7 % possessed fewer than five years of experience, while 38,7 % maintained 5–10 years and 26,6 % had more than ten years. Strategic intervention programs should be implemented because they show the importance of enhancing patient information protection practices.
|
Table 3. Distribution of Knowledge, Awareness, Behavior, and Training on Patient Confidentiality |
|||
|
Variable |
Category |
Frequency (n = 323) |
Percentage (%) |
|
Knowledge of Patient Confidentiality |
Good Knowledge |
136 |
42,2 |
|
Poor Knowledge |
187 |
57,8 |
|
|
Awareness of Confidentiality Principles |
Aware |
98 |
30,3 |
|
Not Aware |
225 |
69,7 |
|
|
Behavior Toward Patient Confidentiality |
Positive Behavior |
95 |
29,5 |
|
Negative Behavior |
228 |
70,5 |
|
|
Confidentiality Training Received |
Yes |
142 |
44,0 |
|
No |
181 |
56,0 |
|
|
Work Setting |
Public Hospital |
170 |
52,6 |
|
Private Hospital |
98 |
30,3 |
|
|
Community Clinic |
55 |
17,1 |
|
|
Years of Experience |
<5 years |
112 |
34,7 |
|
5–10 years |
125 |
38,7 |
|
|
>10 years |
86 |
26,6 |
|
Paired T-test on Patient Confidentiality Training
The paired t-test serves as a method to identify variations between two related groups through pre-intervention and post-intervention measurements for assessing meaningful changes. This evaluation examined patient confidentiality variables through pre-test and post-test examination data to assess the outcome of training and institutional interventions. All final analysis results showed important improvements in variables, where statistical significance was confirmed through p-values of less than 0,05 as shown in table 4 and figure 1. The scores for knowledge about confidentiality principles grew from 5,8 to 7,3 (p = 0,002) showing that participants learned better confidentiality practices. The scores for awareness about confidentiality guidelines achieved significant improvement from 4,9 to 6,7, which was statistically significant with p = 0,004. The research data showed that subjects demonstrated better ethical compliance through behavioral adherence increases from 5,2 to 6,5 (p = 0,006). The measured ethical decision-making capability improved from 6,0 to 7,8 (p = 0,003) and institutional support perception rose from 5.5 to 7.1 (p = 0.005), which reflects heightened workplace attitudes. Structured training programs proved most effective in improving confidentiality standards, as they led to a significant training effectiveness scores from 4,7 to 6,9 (p = 0,001).
|
Table 4. Effect of Training on Knowledge, Awareness, and Behavioral Adherence – Paired t-Test Results |
|||||
|
Variable |
Mean (Pre-Test) |
Mean (Post-Test) |
Mean Difference |
t-Value |
p-Value |
|
Knowledge Score |
5,8 ± 1,2 |
7,3 ± 1,1 |
1,5 |
8,42 |
0,002** |
|
Awareness Score |
4,9 ± 1,4 |
6,7 ± 1,2 |
1,8 |
9,15 |
0,004** |
|
Behavioral Adherence Score |
5,2 ± 1,3 |
6,5 ± 1,0 |
1,3 |
7,98 |
0,006** |
|
Ethical Decision-Making |
6,0 ± 1,5 |
7,8 ± 1,3 |
1,8 |
8,76 |
0,003** |
|
Institutional Support Perception |
5,5 ± 1,4 |
7,1 ± 1,2 |
1,6 |
8,23 |
0,005** |
|
Training Effectiveness |
4,7 ± 1,6 |
6,9 ± 1,3 |
2,2 |
10,34 |
0,001** |
Regression Analysis of Patient Confidentiality-Relating Factors
A statistical method for analyzing the relationship between dependent and independent variables is regression analysis, identifying factors that significantly influence the outcomes. In this analysis, knowledge of patient confidentiality, awareness of confidentiality principles, and behavior toward confidentiality were assessed concerning various independent variablespresented in table 5. The outcomes specify that years of experience positively impact knowledge (B = 0,12, p = 0,018), while confidentiality training has a stronger effect (B = 0,25, p < 0,001), highlighting the importance of formal education in improving knowledge levels. Awareness of confidentiality principles is significantly influenced by age, with younger individuals demonstrating greater awareness (B = 0,18, p = 0,004), and by work setting, where public sector employees exhibit higher awareness (B = 0,20, p < 0,001). Behavior toward confidentiality is significantly improved by training (B = 0,30, p < 0,001) and experience (B = 0,22, p < 0,001), suggesting that both education and practical exposure enhance adherence. However, gender does not have a significant impact on behavior (p = 0,086). These findings emphasize the need for targeted training programs and institutional policies to enhance confidentiality practices in healthcare settings.
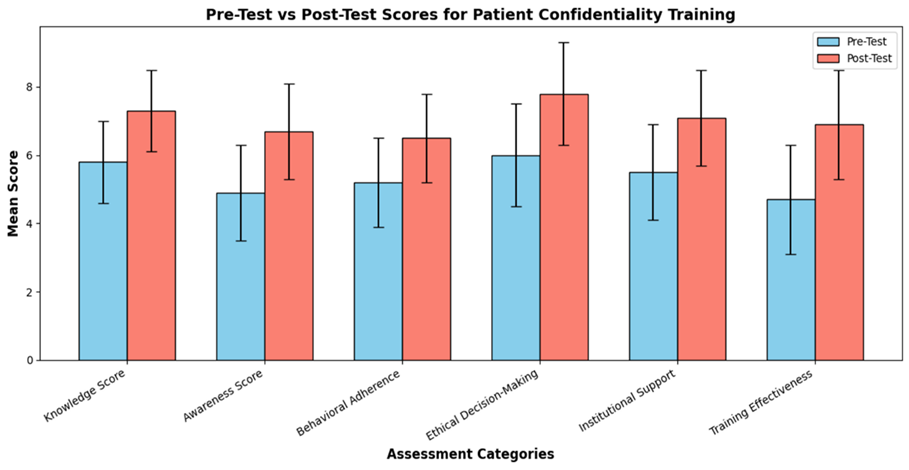
Figure 1. Comparison of Pre-Test and Post-Test Scores for Patient Confidentiality Training
|
Table 5. Predictors of Knowledge, Awareness, and Behavioral Adherence in Patient Confidentiality – Regression Analysis |
|||||||
|
Dependent Variable |
Independent Variable |
B |
β |
t-value |
p-value |
R² |
Interpretation |
|
Knowledge of Patient Confidentiality |
Years of Experience |
0,12 |
0,15 |
2,38 |
0,018* |
0,075 |
Positive effect of experience on knowledge |
|
Confidentiality Training (Yes/No) |
0,25 |
0,30 |
5,12 |
<0,001** |
0,162 |
Training significantly improves knowledge |
|
|
Awareness of Confidentiality Principles |
Age Group (≤40 vs. >40 years) |
0,18 |
0,19 |
2,91 |
0,004** |
0,085 |
Younger age groups show more awareness. |
|
Work Setting (Public vs. Private) |
0,20 |
0,22 |
3,56 |
<0,001** |
0,121 |
Public sector workers are more aware |
|
|
Behavior Toward Confidentiality |
Gender (Male vs. Female) |
0,10 |
0,12 |
1,72 |
0,086 |
0,043 |
Gender does not significantly affect behavior. |
|
Training Received (Yes/No) |
0,30 |
0,35 |
4,98 |
<0,001** |
0,192 |
Training improves behavioral adherence. |
|
|
Experience (>5 years vs. <5 years) |
0,22 |
0,24 |
3,74 |
<0,001** |
0,134 |
More experience improves behavior. |
|
|
Notes: Unstandardized Coefficients-(B), Standardized Coefficients-(β) |
|||||||
DISCUSSION
The healthcare professionals determined patient confidentiality, and the variables that affect adherence in environments with limited resources were investigated in this research. This assessment examines how individuals behave, comprehend, and understand confidentiality protocols. It also evaluates how training approaches affect people’s comprehension. Research indicates institutional rules work environments and experience levels contribute to compliance results while knowledge levels and adherence show major differences. Training programs deliver positive results that build both behavioral commitment to ethical standards and understanding among staff. Health professionals from younger age groups and those working in public health exhibit enhanced awareness and belong to specific demographic institutions. Medical facilities require specific initiatives to strengthen their confidentiality handling protocols based on these findings.
CONCLUSION
Focusing on behavior, knowledge, awareness, and the effect of training in settings with limited resources, the research examines how healthcare workers perceive about patient confidentiality. Most healthcare workers display weak knowledge regarding patient confidentiality, since only 42,2 % demonstrated strong understanding while only 30,3 % knew about the specific rules. The training program improved behavior toward confidentiality, according to survey results because respondents showed positive behavior only 29,5 % of cases at baseline, but training substantially increased their adherence. Behavioral adherence scores and knowledge scores showed significant post-training improvement from 5,2 to 6,5 (p < 0,05) and 5,8 to 7,3 (p < 0,05) respectively. A regression analysis result showed experience (B = 0,22, p < 0,001) and training (B = 0,30, p < 0,001) were prosocial factors for healthcare professionals in following confidentiality policies. Healthcare professionals require immediate institutional regulation and systematic training programs to enhance confidentiality procedures within healthcare organizations. Several research limitations stem from its dependence on respondent-provided information that could produce biased results and its narrow research of a restrained resource environment, which hinders wider application. Future studies need to investigate how both long-term outcomes and advanced digital confidentiality training would perform in multiple healthcare organizations.
REFERENCES
1. Ewuoso C. Patient confidentiality, the duty to protect, and psychotherapeutic care: perspectives from the philosophy of Ubuntu. Theoretical Medicine and Bioethics. 2021 Apr;42(1):41-59. https://doi.org/10.1007/s11017-021-09545-0
2. Balikuddembe JK, Reinhardt JD. Can digitization of health care help low-resourced countries provide better community-based rehabilitation services? Physical therapy. 2020 Feb;100(2):217-24. https://doi.org/10.1093/ptj/pzz162
3. Griffiths F, Watkins JA, Huxley C, Harris B, Cave J, Pemba S, Chipwaza B, Lilford R, Ajisola M, Arvanitis TN, Bakibinga P. Mobile consulting (mConsulting) and its potential for providing access to quality healthcare for populations living in low-resource settings of low-and middle-income countries. Digital health. 2020 Apr;6:2055207620919594. https://doi.org/10.1177/2055207620919594
4. McGraw D, Mandl KD. Privacy protections to encourage the use of health-relevant digital data in a learning health system. NPJ digital medicine. 2021 Jan 4;4(1):2. https://doi.org/10.1038/s41746-020-00362-8
5. Shah SM, Khan RA. Secondary use of electronic health record: Opportunities and challenges. IEEE Access. 2020 Jul 22;8:136947-65. https://doi.org/10.1109/ACCESS.2020.3011099
6. Lustgarten SD, Garrison YL, Sinnard MT, Flynn AW. Digital privacy in mental healthcare: current issues and recommendations for technology use. Current opinion in psychology. 2020 Dec 1;36:25-31. https://doi.org/10.1016/j.copsyc.2020.03.012
7. Gonzalez R, Gasco J, Llopis J. Information and communication technologies and human resources in hospitality and tourism. International Journal of Contemporary Hospitality Management. 2020 Nov 13;32(11):3545-79. https://doi.org/10.1108/IJCHM-04-2020-0272
8. van Boekholt TA, Duits AJ, Busari JO. Health care transformation in a resource-limited environment: exploring the determinants of a good climate for change. Journal of Multidisciplinary Healthcare. 2019 Feb 28:173-82. https://doi.org/10.2147/JMDH.S194180
9. Wagner A, Rieger MA, Manser T, Sturm H, Hardt J, Martus P, Lessing C, Hammer A, WorkSafeMed Consortium E. Luntz MA Rieger H. Sturm A. Wagner A. Hammer T. Manser P. Martus M. Holderried. Healthcare professionals’ perspectives on working conditions, leadership, and safety climate: a cross-sectional study. BMC Health Services Research. 2019 Dec;19:1-4. https://doi.org/10.1186/s12913-018-3862-7
10. Goldstein RF, Walker RE, Teede HJ, Harrison CL, Boyle JA. The healthy pregnancy service to optimize excess gestational weight gain for women with obesity: a qualitative study of health professionals’ perspectives. Journal of Clinical Medicine. 2020 Dec 17;9(12):4073. https://doi.org/10.3390/jcm9124073
11. Nyoni CN, Grobler C, Botma Y. Towards continuing interprofessional education: Interaction patterns of health professionals in a resource-limited setting. PloS one. 2021 Jul 9;16(7):e0253491. https://doi.org/10.1371/journal.pone.0253491
12. Lee K, Lim K, Jung SY, Ji H, Hong K, Hwang H, Lee HY. Perspectives of patients, health care professionals, and developers toward blockchain-based health information exchange: qualitative study. Journal of medical Internet research. 2020 Nov 13;22(11):e18582. https://doi.org/10.2196/18582
13. Enaizan O, Zaidan AA, Alwi NH, Zaidan BB, Alsalem MA, Albahri OS, Albahri AS. Electronic medical record systems: Decision support examination framework for individual, security, and privacy concerns using multi-perspective analysis. Health and Technology. 2020 May;10:795-822. https://doi.org/10.1007/s12553-018-0278-7
14. Mogre V, Johnson NA, Tzelepis F, Paul C. Barriers to diabetic self‐care: A qualitative study of patients’ and healthcare providers’ perspectives. Journal of Clinical Nursing. 2019 Jun;28(11-12):2296-308. https://doi.org/10.1111/jocn.14835
15. Esmaeilzadeh P, Mirzaei T. The potential of blockchain technology for health information exchange: experimental study from patients’ perspectives. Journal of medical Internet research. 2019 Jun 20;21(6):e14184. https://doi.org/10.2196/14184
16. Wei H, Corbett RW, Ray J, Wei TL. A culture of caring: the essence of healthcare interprofessional collaboration. Journal of interprofessional care. 2020 May 3;34(3):324-31. https://doi.org/10.1080/13561820.2019.1641476
17. Basholli A, Lagkas T, Bath PA, Eleftherakis G. Sensor-based platforms for remote management of chronic diseases in developing regions: a qualitative approach examining the perspectives of healthcare professionals. Health informatics journal. 2021 Jan;27(1):1460458220979350. https://doi.org/10.1177/1460458220979350
FINANCING
None.
CONFLICT OF INTEREST
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
AUTHORSHIP CONTRIBUTION
Conceptualization: Ved vrat verma, Samir Samal, RenukaJyothi S.
Data curation: Ved vrat verma, Samir Samal, RenukaJyothi S.
Formal analysis: Ved vrat verma, Samir Samal, RenukaJyothi S.
Research: Jaya Ved vrat verma, Samir Samal, RenukaJyothi S.
Methodology: Ved vrat verma, Samir Samal, RenukaJyothi S.
Project management: Ved vrat verma, Samir Samal, RenukaJyothi S.
Resources: Ved vrat verma, Samir Samal, RenukaJyothi S.
Software: Ved vrat verma, Samir Samal, RenukaJyothi S.
Supervision: Ved vrat verma, Samir Samal, RenukaJyothi S.
Validation: Ved vrat verma, Samir Samal, RenukaJyothi S.
Display: Ved vrat verma, Samir Samal, RenukaJyothi S.
Drafting - original draft: Ved vrat verma, Samir Samal, RenukaJyothi S.
Writing: Ved vrat verma, Samir Samal, RenukaJyothi S.